Downloaded 139 times











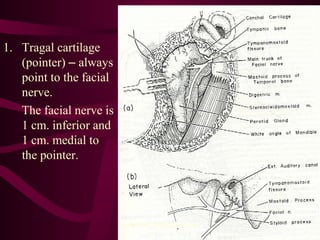


The document discusses parotid tumors and parotidectomy surgery. It provides information on the types and characteristics of benign and malignant parotid tumors, including the most common types. Evaluation, treatment, and complications of parotid surgery are described, with key points on identifying and preserving the facial nerve during parotidectomy procedures.























































































