Downloaded 140 times


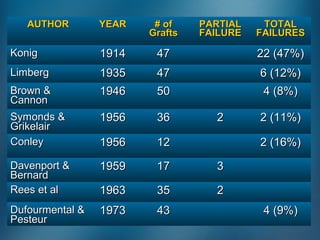



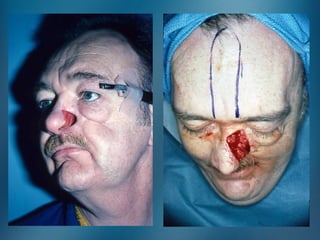






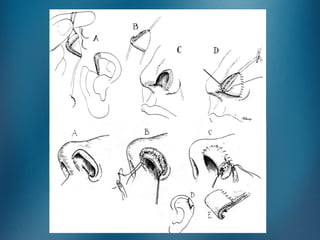
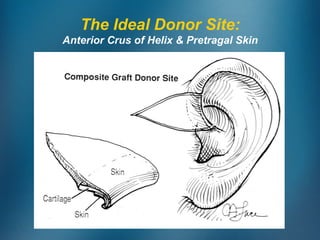
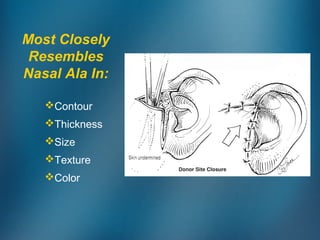



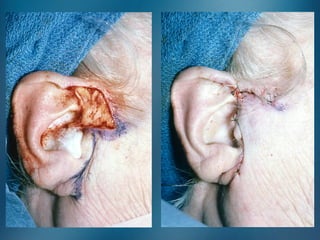



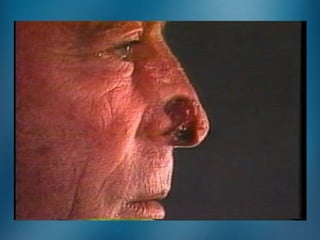









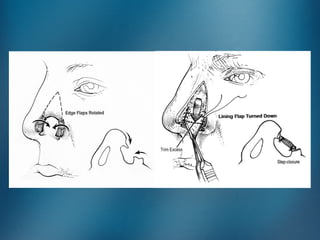
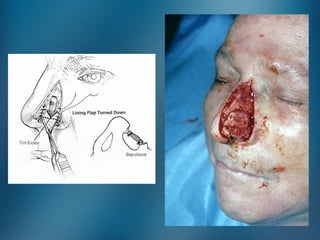
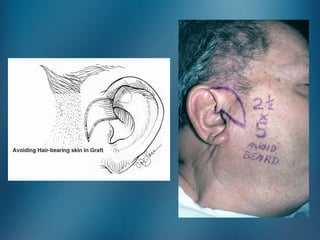
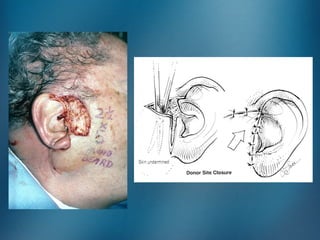

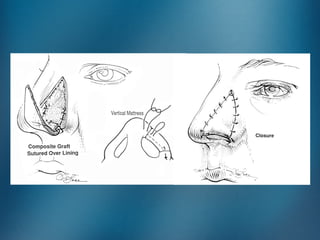


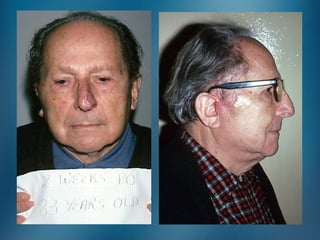

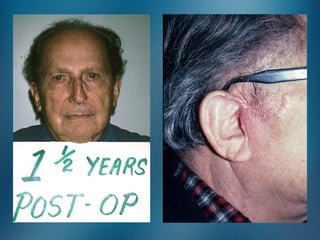





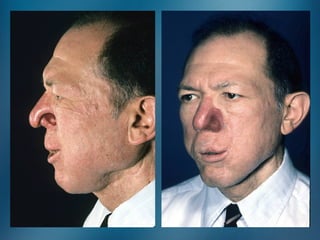

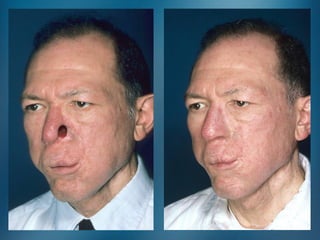
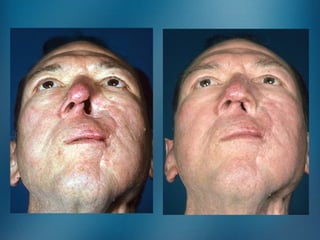








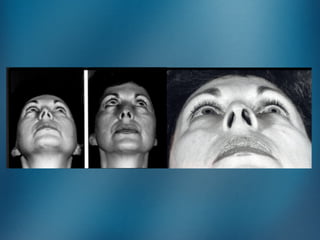
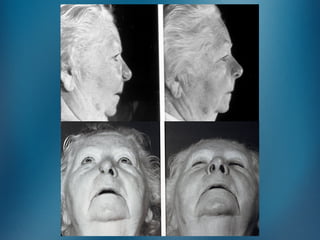


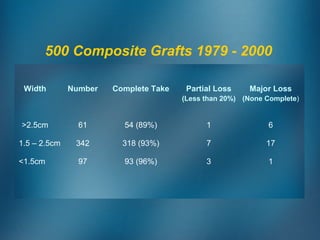
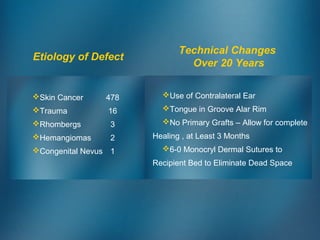



This document discusses nasal reconstruction using composite chondrocutaneous grafts. It provides a brief history of composite grafts, noting their phases of revascularization. Tables show success rates from various studies ranging from 47% to 12% partial failure and up to 16% total failure. A 2cm graft has a 90-95% survival rate. The ideal donor site is the anterior crus of the helix and pretragal skin. Factors for success include graft size over 1.5cm, atraumatic handling, a well-vascularized turn-down flap, and patient cooperation to not smoke, chew, or talk. Advantages over flaps include a one-stage operation, superior donor site, patient comfort, and




























































































