Downloaded 24 times

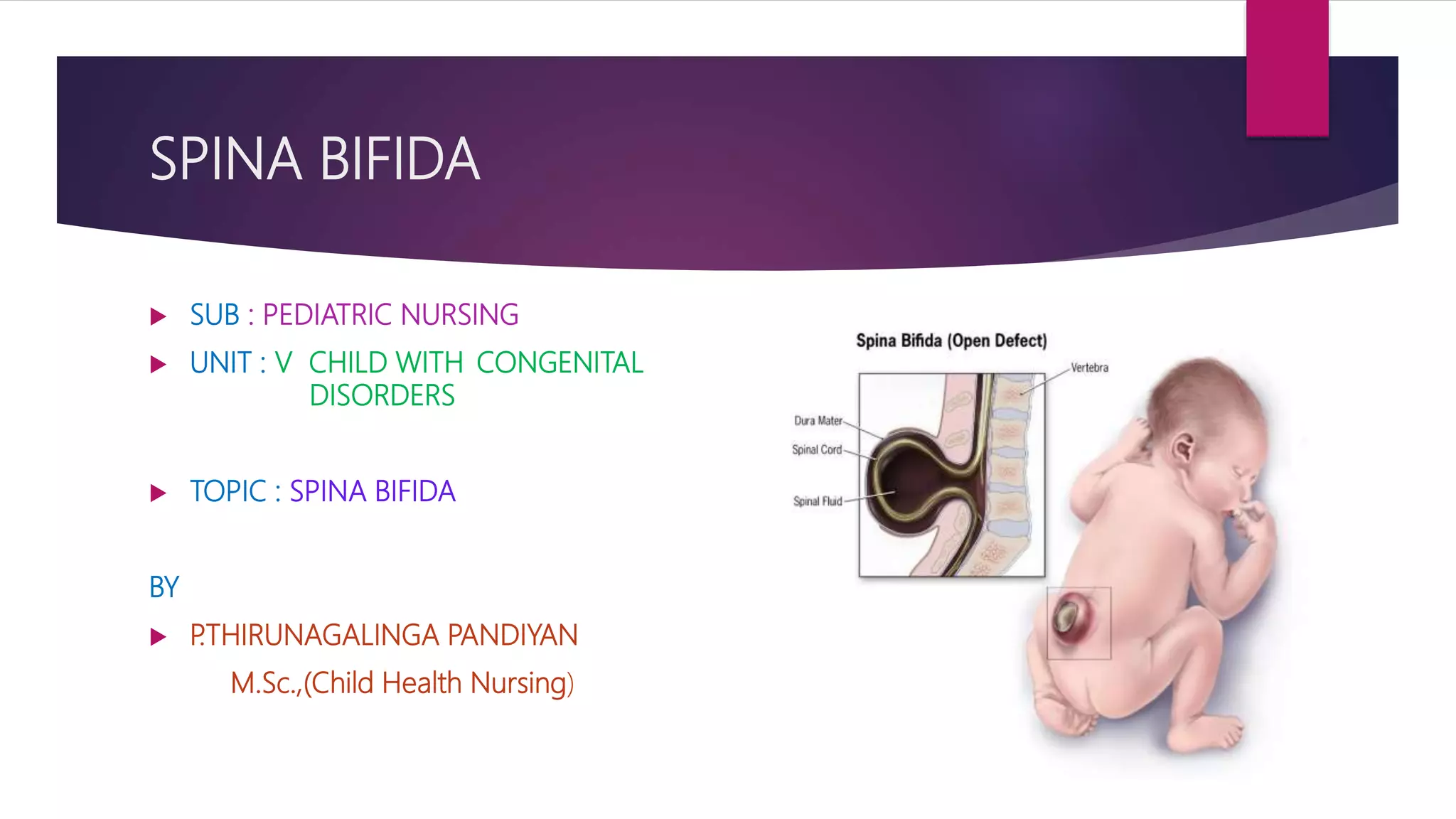

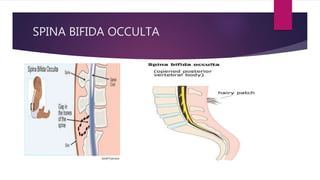





Spina bifida is a birth defect where the spine and spinal cord do not form properly. It can range from mild to severe, causing physical and intellectual disabilities. It occurs when the neural tube fails to close fully during early embryonic development. The three main types are spina bifida occulta, meningocele, and myelomeningocele. Treatment involves surgery to repair the spine and prevent infection, along with physical therapy, bladder and bowel management, and orthopedic care. Prevention focuses on adequate folic acid intake before and during pregnancy to help reduce risks.