Downloaded 524 times
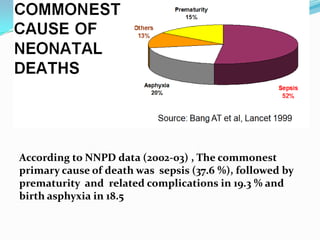
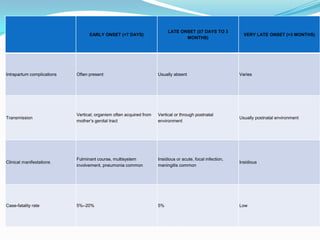
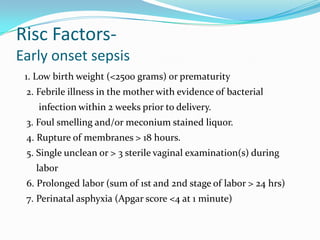
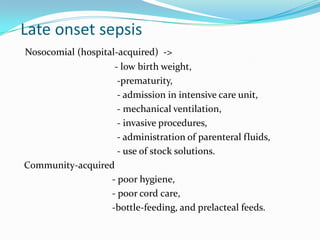
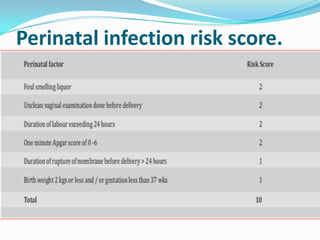
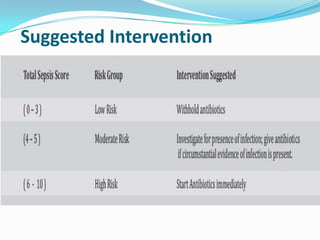
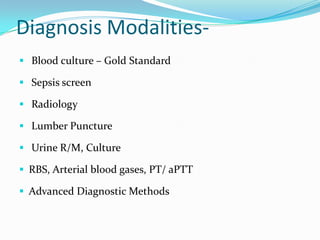
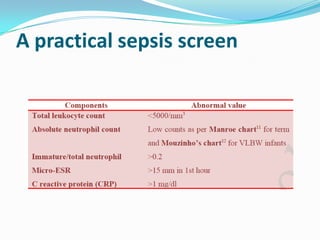
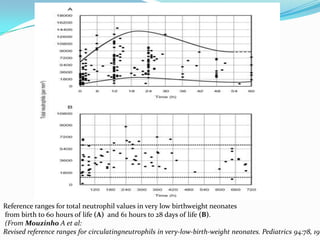
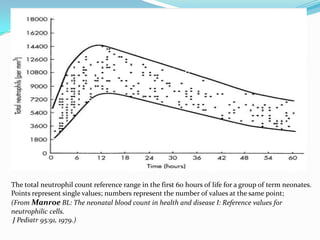
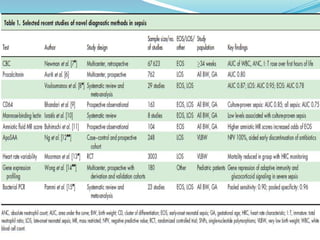
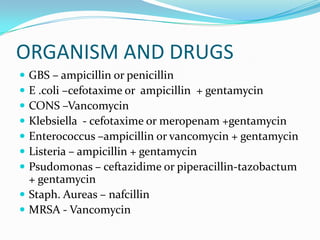
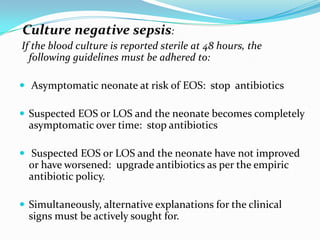

This document discusses recent advances in neonatal septicemia. It begins by defining neonatal septicemia and describing the types, including early onset sepsis within 72 hours of birth and late onset sepsis from 3-90 days of life. It then discusses the epidemiology, risk factors, clinical presentation and diagnostic evaluation. Key diagnostic tests discussed include blood cultures, sepsis screens, lumbar puncture and novel biomarkers. Management of neonatal septicemia includes supportive care and administration of empiric and targeted antibiotic therapy guided by culture results.



































































![Sepsis neonatal [autoguardado]](https://cdn.slidesharecdn.com/ss_thumbnails/sepsisneonatalautoguardado-170318103240-thumbnail.jpg?width=640&height=640&fit=bounds)














![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




