- Neonatal seizures, febrile seizures, CNS infections, and strokes are common neurological conditions seen in pediatrics.
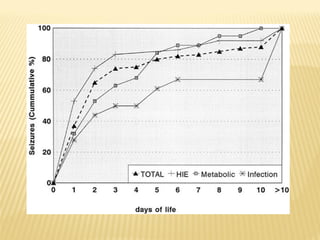
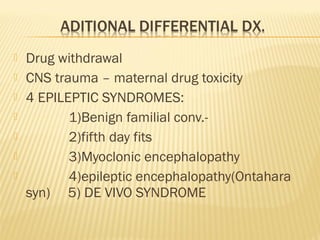
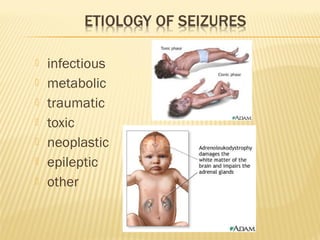
- Common etiologies of neonatal seizures include hypoxic-ischemic encephalopathy, congenital CNS anomalies, intracranial hemorrhage, and electrolyte or metabolic abnormalities.
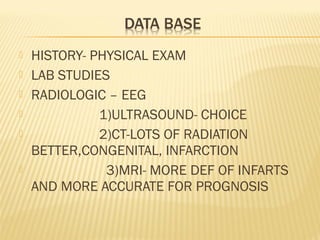
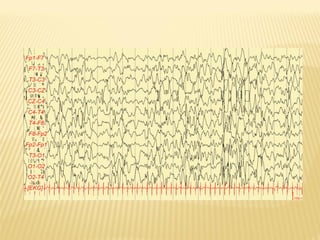
- Evaluation involves history, physical exam, lab studies, and neuroimaging like EEG, ultrasound, CT, or MRI depending on the situation.
- Treatment involves anticonvulsants tailored to the specific condition, with phenobarbital, phenytoin, and lorazepam as first line options for status epilepticus.