



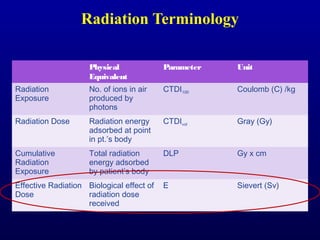




























The document discusses the risks and benefits of ionizing radiation in medical diagnostic imaging, emphasizing the importance of balancing radiation exposure with diagnostic quality. It reviews radiation sources, dose reduction techniques, and controversies surrounding medical imaging radiation. It also highlights epidemiological studies on cosmic radiation exposure for airline personnel and the challenges in establishing links between radiation exposure and cancer.





























































































