Downloaded 36 times

![Cancer incidence (1950-1984) and
A-Bomb radiation exposure
DS86 maternal uterine dose (Gy)
0 0.01-0.29 0.30-0.59 >0.6
Mean dose (Gy) 0.000 0.087 0.416 1.372
No. at risk 710 682 129 109
Person-Years 21770 21659 4095 3287
Cancer cases 5 7 3 3
Adjusted rate per 100,000 22.4 32.5 77.8 97.0
Esstimated RR 1.00 1.24 2.18 4.78
[1.01-2.10] [1.06-6.32] 1.19-7.93](https://image.slidesharecdn.com/2014radiation-140318190226-phpapp02/85/2014-radiation-17-320.jpg)
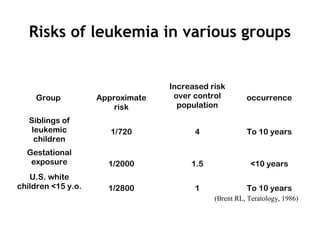
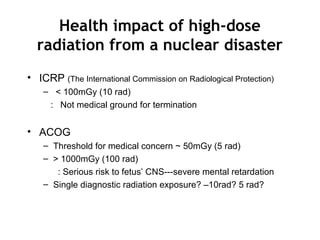
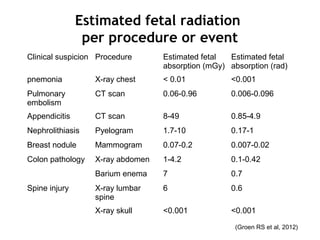
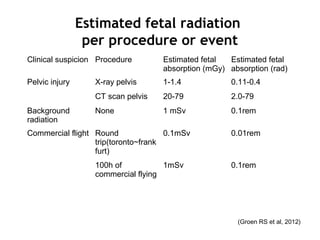
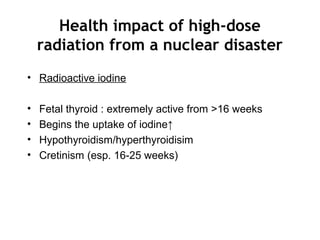
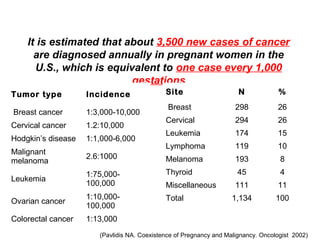
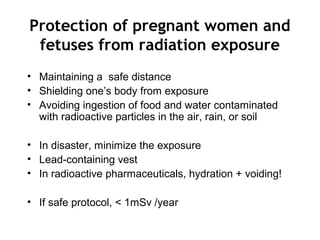
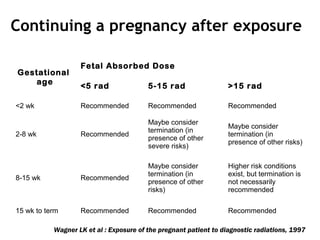

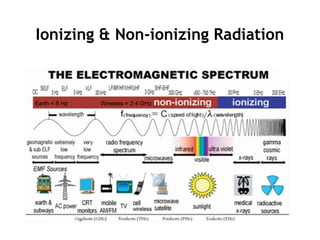
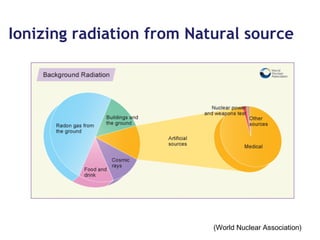
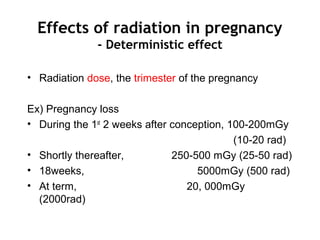
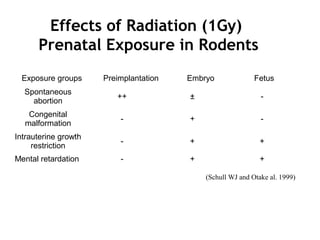
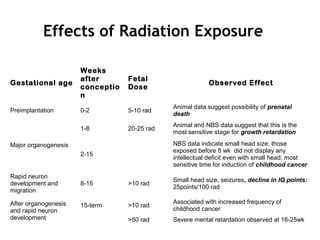
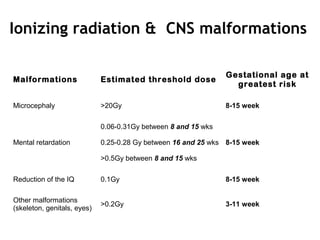
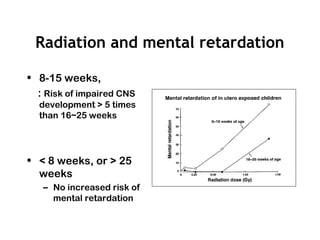
This document discusses the risks of ionizing radiation exposure during pregnancy. It defines ionizing radiation and teratogens, and outlines the critical periods of pregnancy when radiation exposure could impact fetal development. Exposure to high doses of radiation can increase risks of pregnancy loss, malformations, growth restriction, and cancer. The effects are dependent on radiation dose and gestational timing of exposure. Diagnostic procedures pose small risks but high doses over 50mGy or 100rad may cause mental retardation. Protecting the pregnant woman from unnecessary radiation is recommended.























































































