PRESSURE TESTING PERMIT Form # HSEQ - PTP Rev 2 -.docx

1. Project Information: (To be filled by initiator/originator) Project Name: Permit No.: Project Location: Requesting Contractor/Company 2. Permit Issuance Details: (To be filled by initiator/originator) THIS PERMIT IS ONLY FOR ONE TEST AND IS NOT EXTENDABLE Description of Task: Permit Validity: Time (from): __________Hrs. Time (To): __________Hrs. Date: Design Pressure of Pipeline: Operating Pressure: Testing Pressure: Pressure Time: 3. Pressure Testing Details: (To be filled by initiator/originator) Type of Work Request ☐ Hydrostatic ☐ Pneumatic ☐ Gravity Testing ☐ Other : Type of Equipment testing: ☐ Pipeline ☐ GRP ☐ AC ☐ others: ☐ Tanks ☐ Hose ☐ Other(s) Dimensions: Pipeline/Tank/Hose ☐ Diameter: ☐ Thickness: ☐ Length: ☐ Other(s): Attachment(s): ☐ Plan ☐ Sketch ☐ Drawing (approved) ☐ Method Statement & Risk Assessment ☐ Authority Approvals (NOCs) ☐ Road Traffic Approval (if applicable) ☐ Other(s) 4. Prerequisites: (To be filled by initiator/originator and verified by Evaluator) Checks Yes-No-NA Checks Yes-No-NA Is the segment of pipeline under testing isolated from service by closing nearest valves? ☐ ☐ ☐ Risk assessment/ method statement developed, approved and communicated? ☐ ☐ ☐ Is the Liquid/Gas vented/removed from the pipeline? ☐ ☐ ☐ Testing & monitoring of the environment prior to entry? ☐ ☐ ☐ Test Head and End plug/end point are properly sealed/secured/tighten. ☐ ☐ ☐ Emergency response procedure and rescue plan are developed & communicated? ☐ ☐ ☐ Is Air vented completely by pumping and filling the water in the testing segment pipeline without pressurizing? ☐ ☐ ☐ Operatives are trained and competent? ☐ ☐ ☐ Pressure testing equipment in good condition with available safe guards ☐ ☐ ☐ Provision of vigilance supervision? ☐ ☐ ☐ Flexible pipe/hose are in good condition and connections are safely clamped ☐ ☐ ☐ Proper barricade and signage are posted? ☐ ☐ ☐ Pressure testing gauge have valid calibration. ☐ ☐ ☐ Safe means of access/egress provided? ☐ ☐ ☐ Pressure testing gauge/ valve are in safe & accessible place outside restricted/isolated area ☐ ☐ ☐ Means of communication available? ☐ ☐ ☐ Is the testing pipeline/vessel/tank are properly isolated ☐ ☐ ☐ Electrical equipment & connections safe? ☐ ☐ ☐ Is confined space PTW required & obtained? ☐ ☐ ☐ Other(s) ☐ ☐ ☐ 5. Acknowledgement by Initiator and Evaluator: ☐ Acknowledge that all above precautions have been taken. These have also been fully explained to the operatives, and I consider them competent to do it safely. Initiator/Originator Name: Designation: Signature: Date /Time: ☐ Acknowledge that I have checked above control measures and consider the work area safe to carry out the activity Evaluator (HSE Team): Designation: Signature: Date /Time Comments (if any): 6. Authorization (PM/CM): Name: Designation: Signature: Date /Time:

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to PRESSURE TESTING PERMIT Form # HSEQ - PTP Rev 2 -.docx
Similar to PRESSURE TESTING PERMIT Form # HSEQ - PTP Rev 2 -.docx (20)
More from Dwarika Bhushan Sharma
More from Dwarika Bhushan Sharma (20)
Recently uploaded
Recently uploaded (20)
PRESSURE TESTING PERMIT Form # HSEQ - PTP Rev 2 -.docx
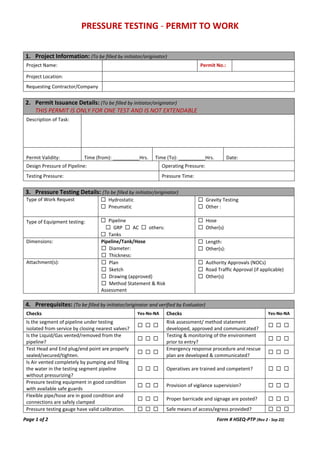
- 1. PRESSURE TESTING - PERMIT TO WORK Page 1 of 2 Form # HSEQ-PTP (Rev 2 - Sep 22) 1. Project Information: (To be filled by initiator/originator) Project Name: Permit No.: Project Location: Requesting Contractor/Company 2. Permit Issuance Details: (To be filled by initiator/originator) THIS PERMIT IS ONLY FOR ONE TEST AND IS NOT EXTENDABLE Description of Task: Permit Validity: Time (from): __________Hrs. Time (To): __________Hrs. Date: Design Pressure of Pipeline: Operating Pressure: Testing Pressure: Pressure Time: 3. Pressure Testing Details: (To be filled by initiator/originator) Type of Work Request ☐ Hydrostatic ☐ Pneumatic ☐ Gravity Testing ☐ Other : Type of Equipment testing: ☐ Pipeline ☐ GRP ☐ AC ☐ others: ☐ Tanks ☐ Hose ☐ Other(s) Dimensions: Pipeline/Tank/Hose ☐ Diameter: ☐ Thickness: ☐ Length: ☐ Other(s): Attachment(s): ☐ Plan ☐ Sketch ☐ Drawing (approved) ☐ Method Statement & Risk Assessment ☐ Authority Approvals (NOCs) ☐ Road Traffic Approval (if applicable) ☐ Other(s) 4. Prerequisites: (To be filled by initiator/originator and verified by Evaluator) Checks Yes-No-NA Checks Yes-No-NA Is the segment of pipeline under testing isolated from service by closing nearest valves? ☐ ☐ ☐ Risk assessment/ method statement developed, approved and communicated? ☐ ☐ ☐ Is the Liquid/Gas vented/removed from the pipeline? ☐ ☐ ☐ Testing & monitoring of the environment prior to entry? ☐ ☐ ☐ Test Head and End plug/end point are properly sealed/secured/tighten. ☐ ☐ ☐ Emergency response procedure and rescue plan are developed & communicated? ☐ ☐ ☐ Is Air vented completely by pumping and filling the water in the testing segment pipeline without pressurizing? ☐ ☐ ☐ Operatives are trained and competent? ☐ ☐ ☐ Pressure testing equipment in good condition with available safe guards ☐ ☐ ☐ Provision of vigilance supervision? ☐ ☐ ☐ Flexible pipe/hose are in good condition and connections are safely clamped ☐ ☐ ☐ Proper barricade and signage are posted? ☐ ☐ ☐ Pressure testing gauge have valid calibration. ☐ ☐ ☐ Safe means of access/egress provided? ☐ ☐ ☐
- 2. PRESSURE TESTING - PERMIT TO WORK Page 2 of 2 Form # HSEQ-PTP (Rev 2 - Sep 22) Pressure testing gauge/ valve are in safe & accessible place outside restricted/isolated area ☐ ☐ ☐ Means of communication available? ☐ ☐ ☐ Is the testing pipeline/vessel/tank are properly isolated ☐ ☐ ☐ Electrical equipment & connections safe? ☐ ☐ ☐ Is confined space PTW required & obtained? ☐ ☐ ☐ Other(s) ☐ ☐ ☐ 5. Acknowledgement by Initiator and Evaluator: ☐ Acknowledge that all above precautions have been taken. These have also been fully explained to the operatives, and I consider them competent to do it safely. Initiator/Originator Name: Designation: Signature: Date /Time: ☐ Acknowledge that I have checked above control measures and consider the work area safe to carry out the activity Evaluator (HSE Team): Designation: Signature: Date /Time Comments (if any): 6. Authorization (PM/CM): Name: Designation: Signature: Date /Time: 7. Completion/Cancelation of Permit: ☐ Acknowledge that the area have been restored to a safe and orderly condition. Initiator Signature: Time: ☐ Acknowledge that I have checked the area and been restored to a safe and orderly condition. Evaluator Signature : Time: