Downloaded 20 times
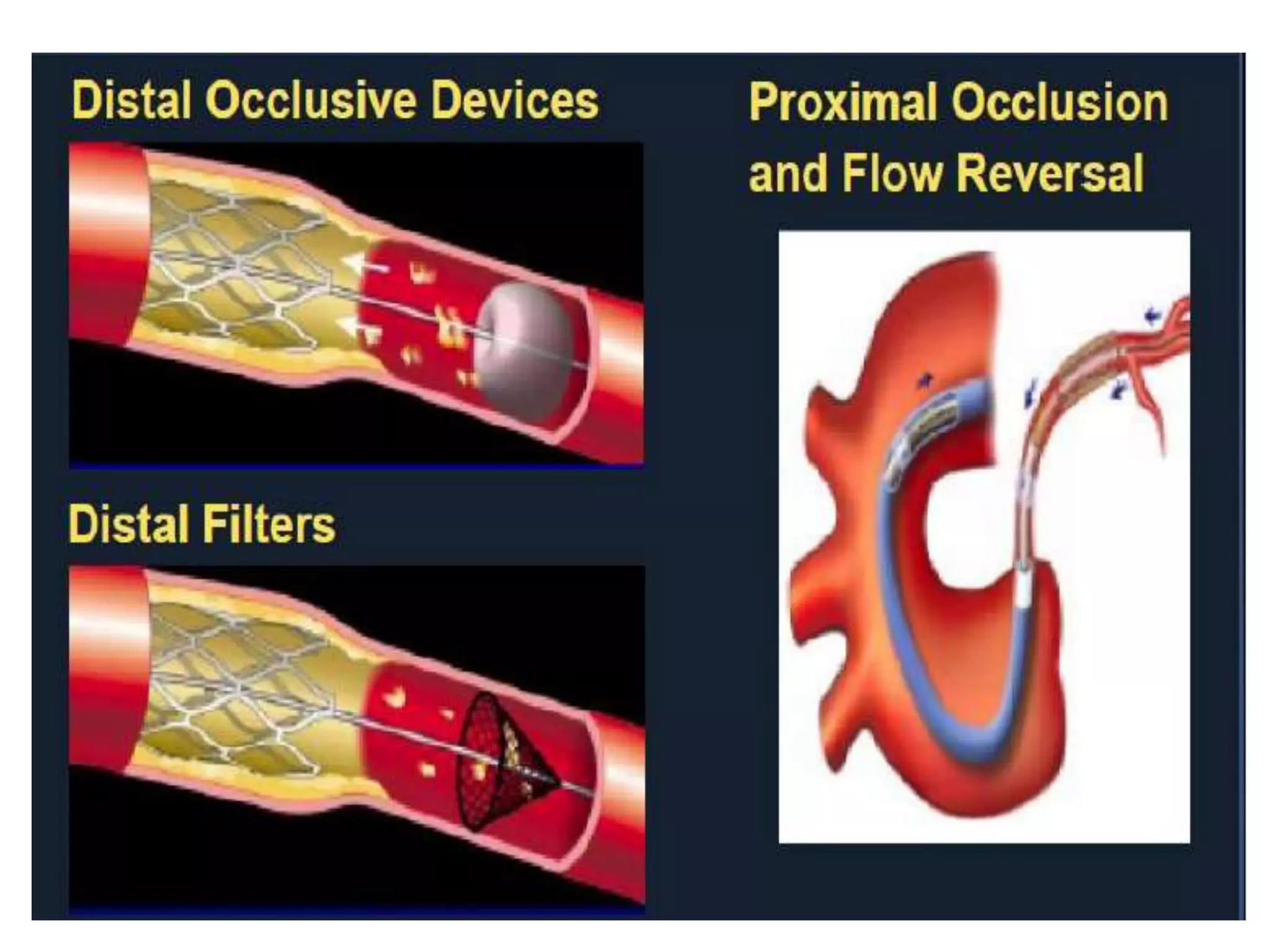





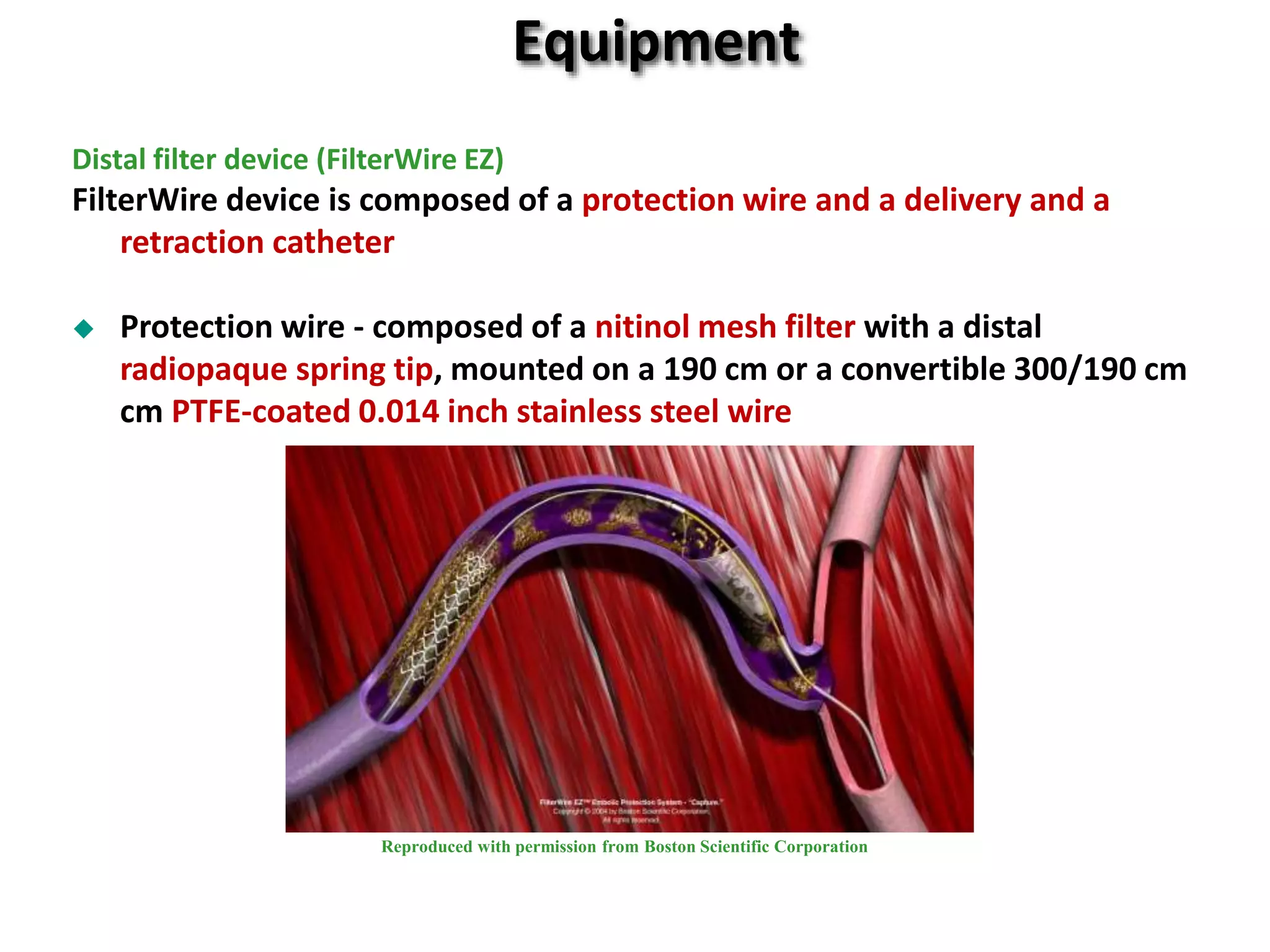





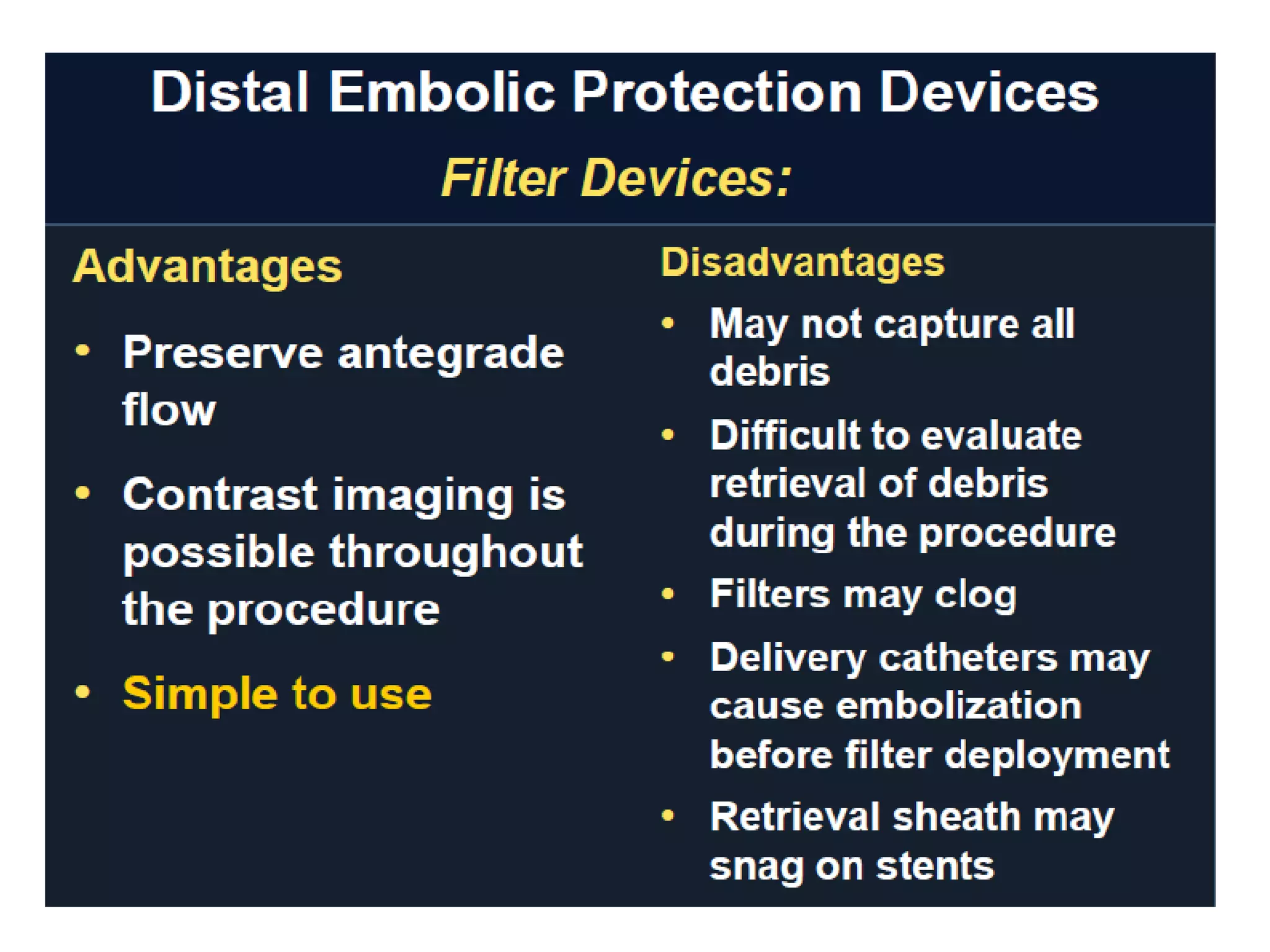




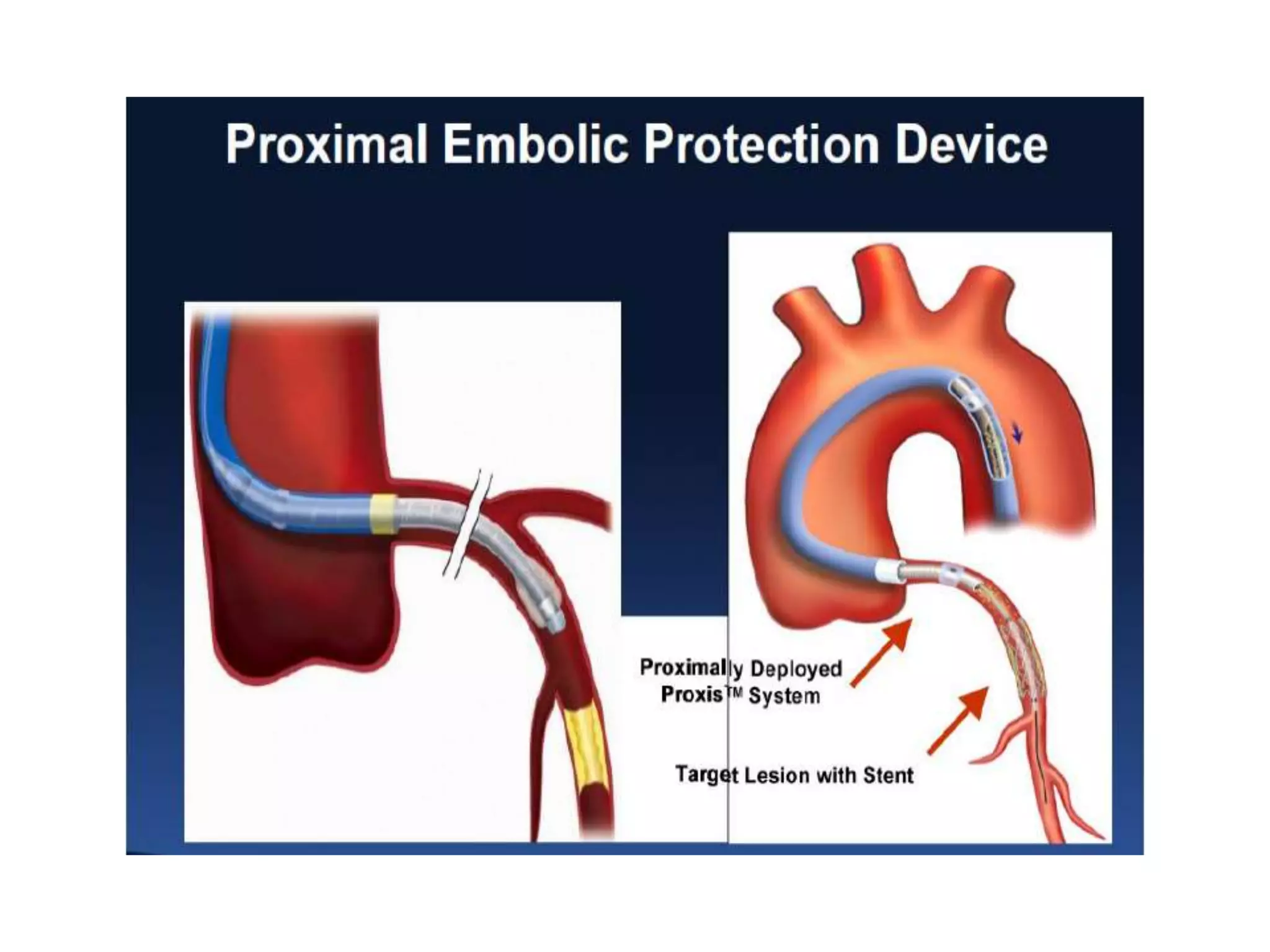




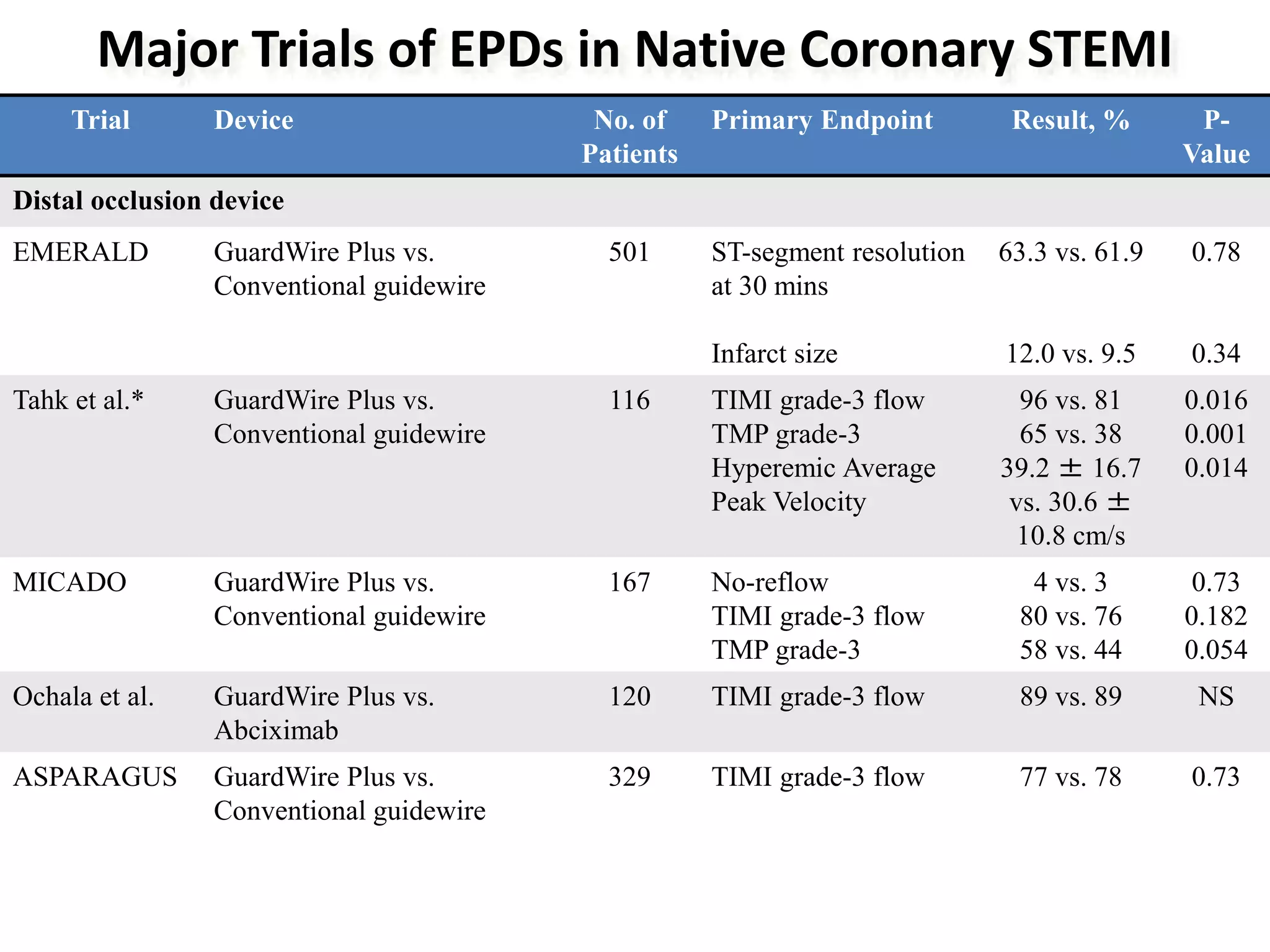










Distal balloon occlusion devices and distal filter devices are the main types of embolic protection devices (EPDs) used during percutaneous coronary intervention (PCI). Distal balloon occlusion devices use a balloon to occlude blood flow distal to the lesion during PCI, while distal filter devices use a nitinol mesh filter to capture debris without interrupting blood flow. Major trials have shown the benefits of EPDs for saphenous vein graft interventions and for STEMI patients undergoing PCI. EPD selection depends on lesion location and vessel characteristics. EPDs are recommended for saphenous vein graft PCI but their routine use is not supported for native coronary artery PCI.









































































