Downloaded 289 times
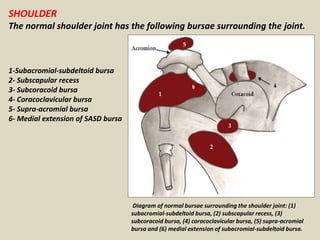











This document discusses various bursae in the body, including those around the shoulder, knee, and other joints. It provides details on the anatomy and locations of bursae and describes imaging findings of normal and pathological bursae. Key points include: - Bursae are fluid-filled sacs that reduce friction between tissues like tendons and bones. They can communicate with joints or be separate. - Common shoulder bursae include the subacromial-subdeltoid bursa and subcoracoid bursa. MRI is useful for identifying bursal inflammation or fluid from rotator cuff tears. - Around the knee, the superficial and deep infrapatellar burs





































![knee_pres_1[1]](https://cdn.slidesharecdn.com/ss_thumbnails/kneepres11-1272133291-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












