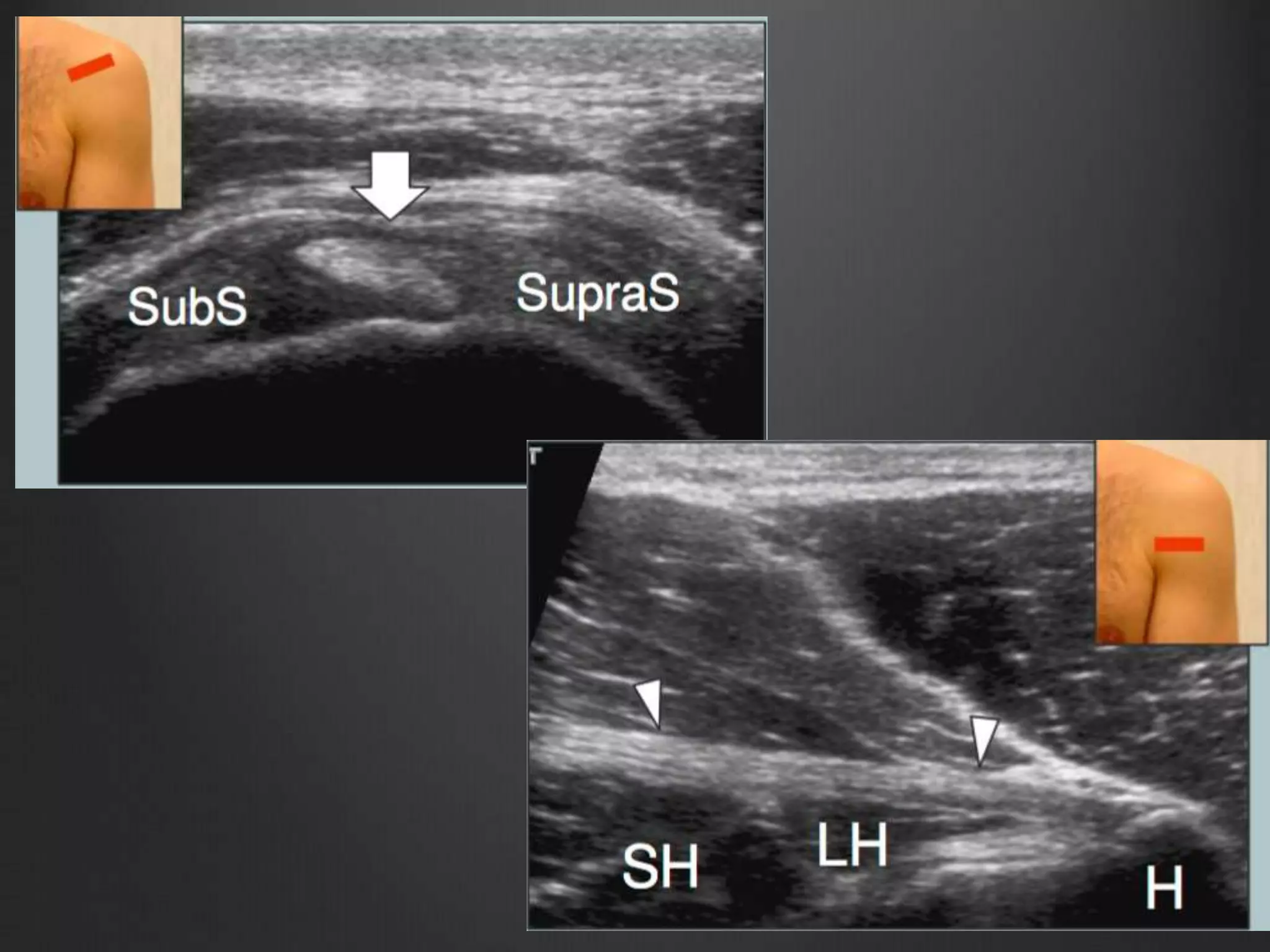
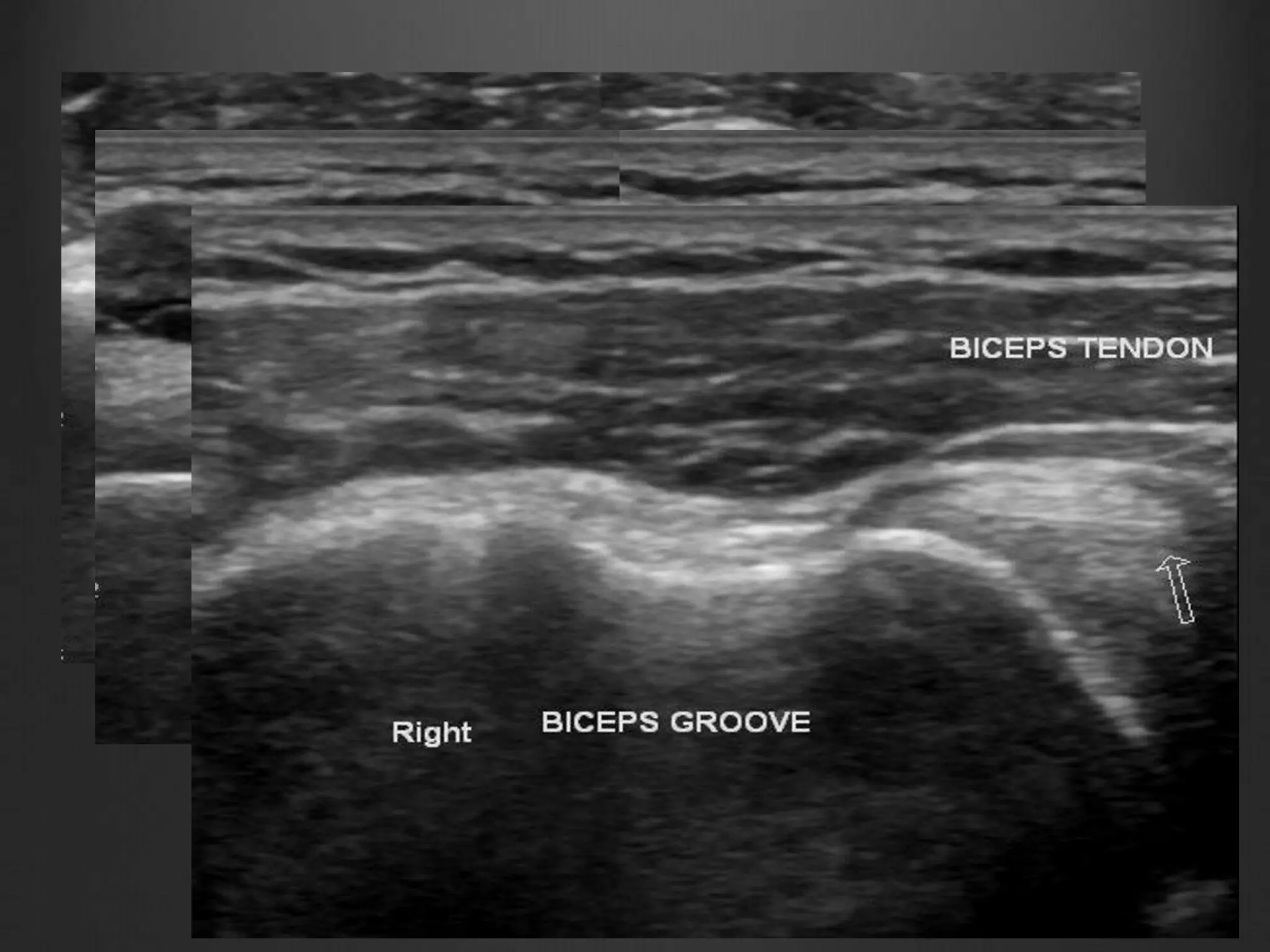
This document discusses ultrasound evaluation of the shoulder. It begins with shoulder anatomy including the ball and socket glenohumeral joint formed by the humerus, scapula, and clavicle. It describes scanning techniques for evaluating the rotator cuff muscles, long head of the biceps tendon, subscapularis tendon, supraspinatus tendon, rotator interval, acromioclavicular joint, and impingement testing. Common pathologies like rotator cuff tears, biceps tendon subluxation, tendinosis, calcific tendinitis, and labral cysts are described. Examples of departmental cases demonstrate ultrasound findings of biceps































































































![Shoulder_joint_and_applied_aspects[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/shoulderjointandappliedaspects1-240425164911-e75cbd49-thumbnail.jpg?width=640&height=640&fit=bounds)
































