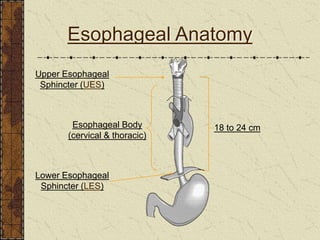
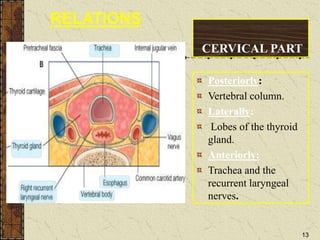
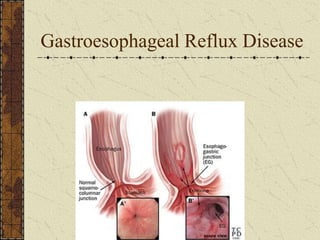
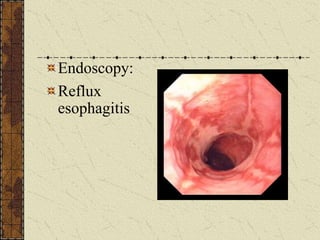
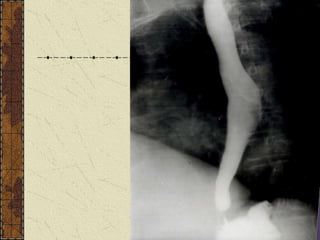
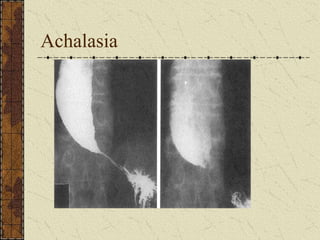
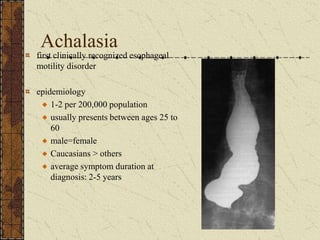
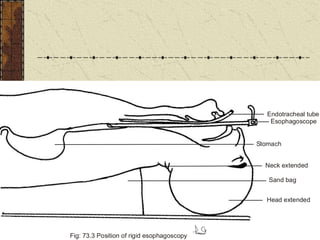
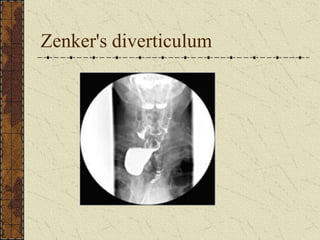
The document discusses the anatomy and physiology of the esophagus. It describes the esophagus as a muscular tube that extends from the pharynx to the stomach. It has three portions - cervical, thoracic, and abdominal. The document outlines the relations of the esophagus in each portion and describes conditions like dysphagia, esophageal sphincters, gastroesophageal reflux disease, achalasia, Zenker's diverticulum and their clinical features and treatments.