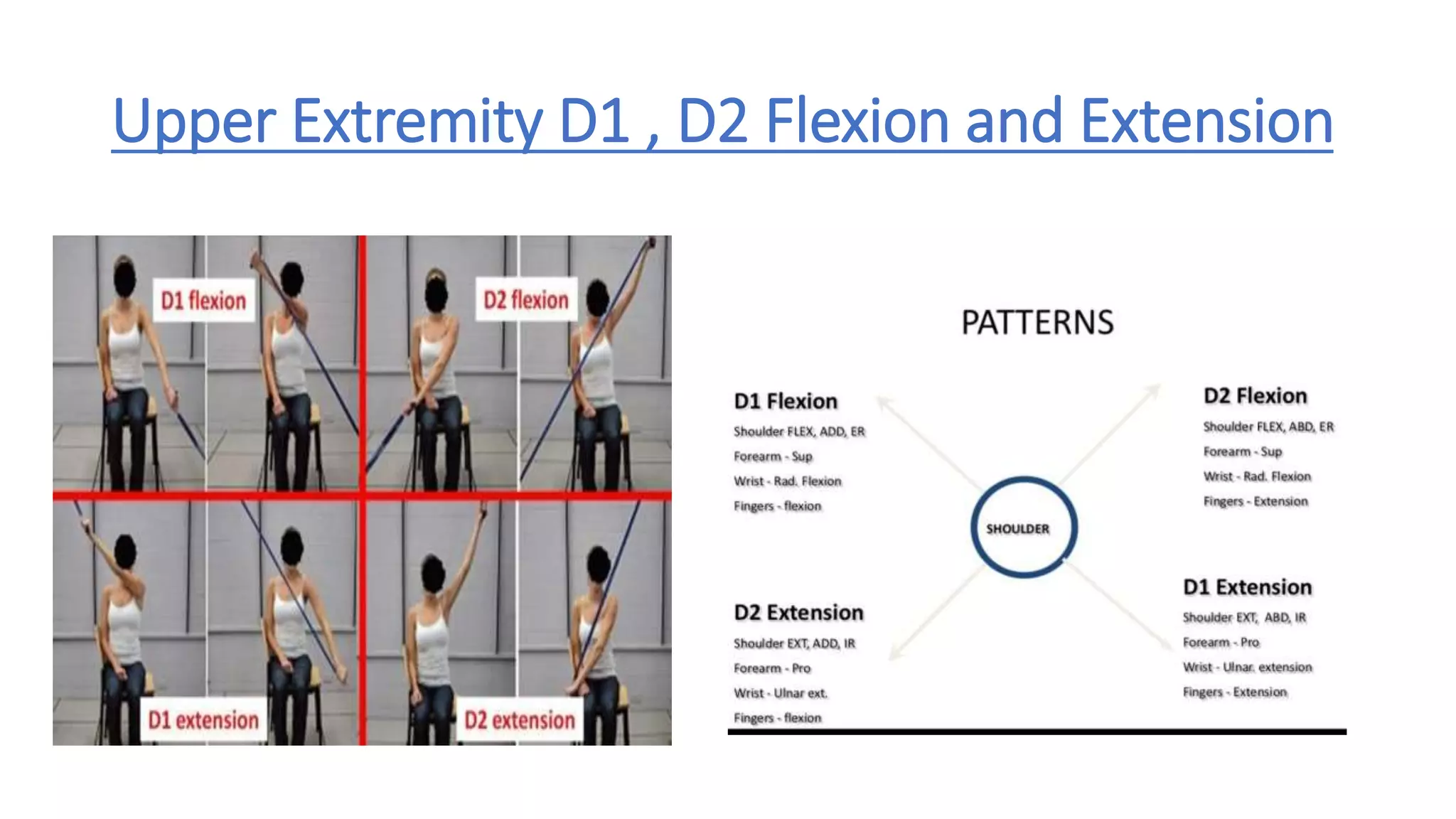
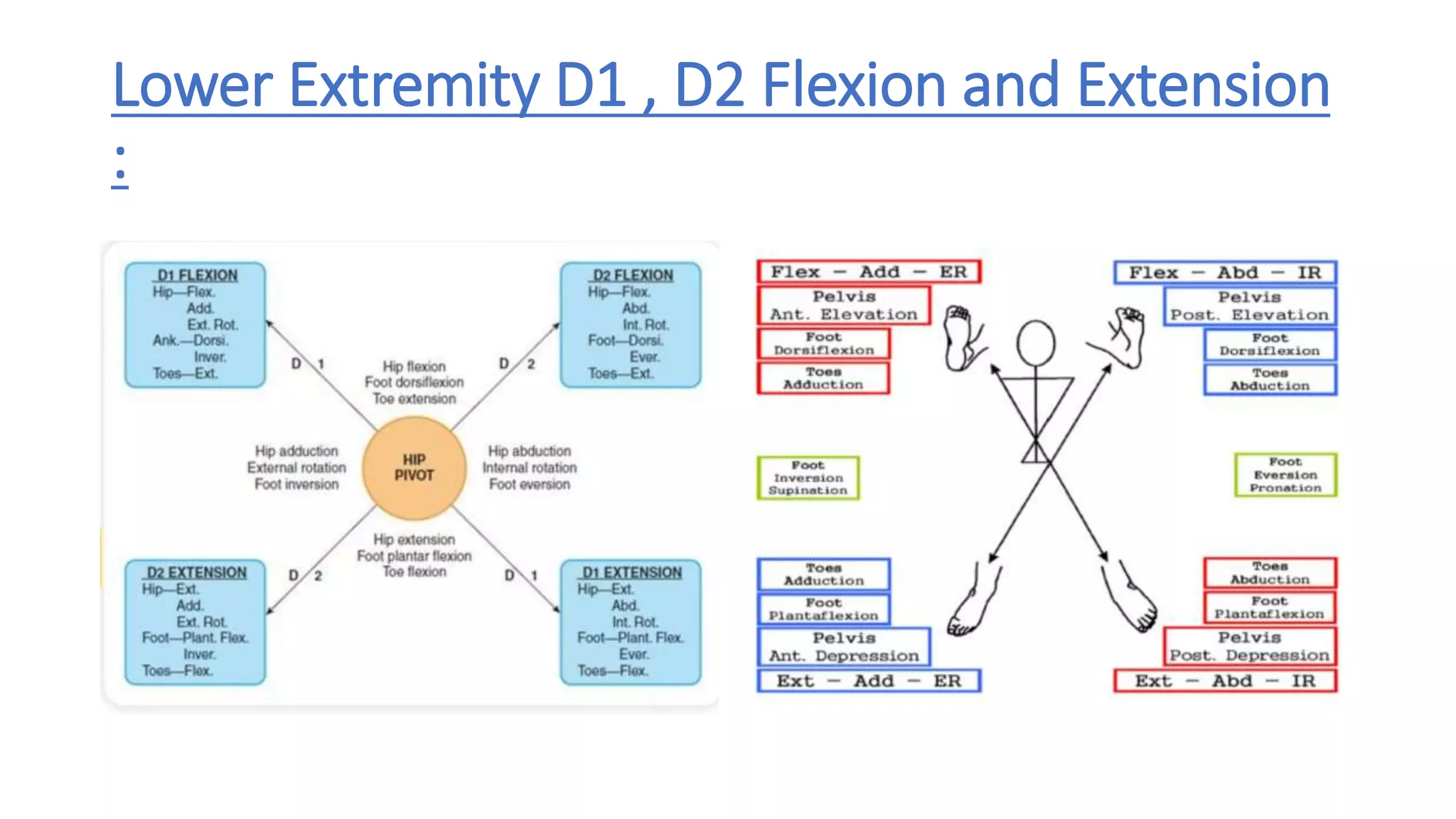
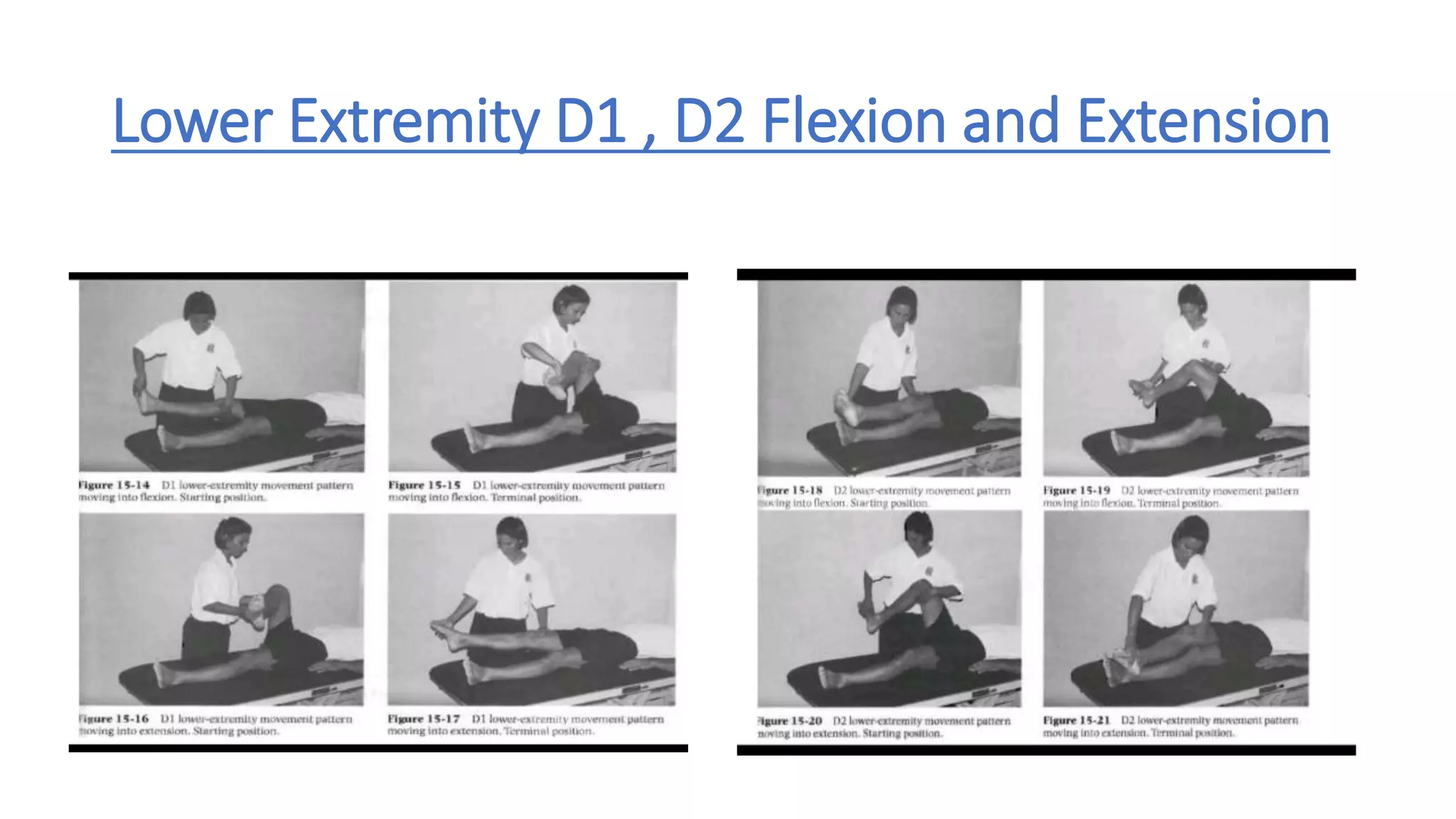
Proprioceptive neuromuscular facilitation (PNF) is a stretching technique developed in the 1940s to enhance both active and passive range of motion. It uses patterns of diagonal and functional movements along with techniques like isometric contractions and combinations of passive stretching and muscle facilitation. The main PNF techniques are rhythmic initiation, repeated contraction, slow reversal, and contract-relax which aim to increase muscle strength and flexibility through repetition. PNF can be used to treat conditions involving muscle weakness or spasticity such as after a stroke.