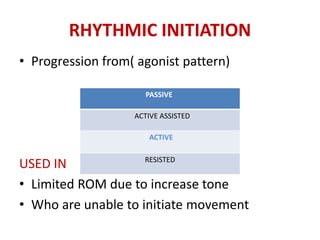
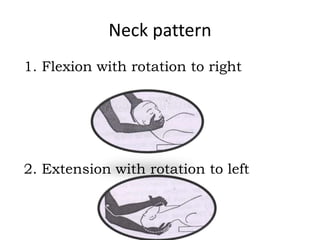
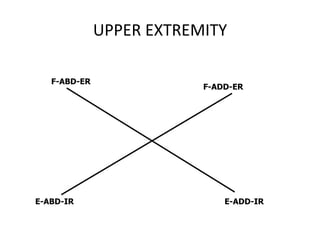
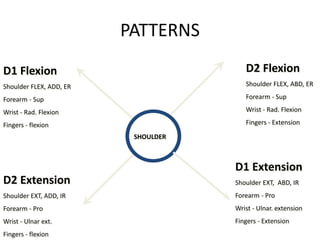
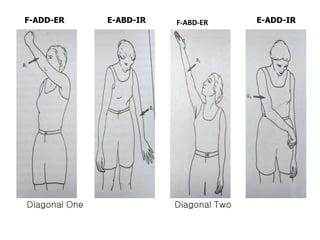
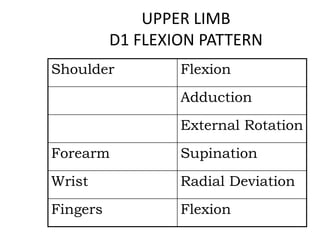
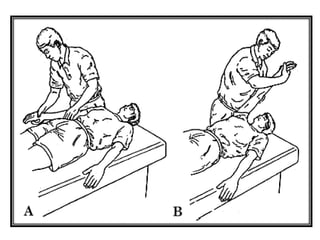
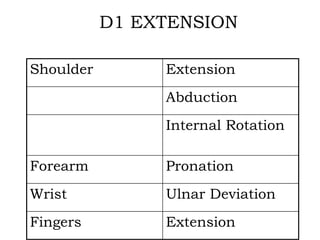
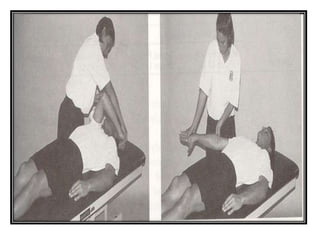
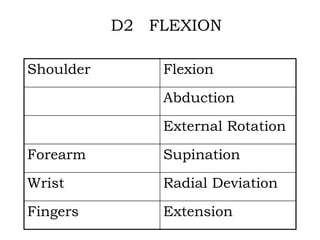
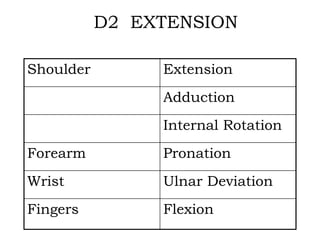
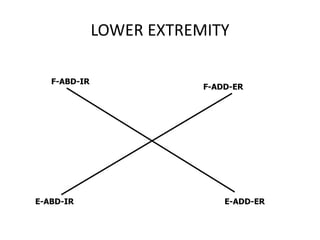
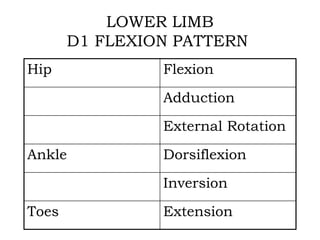
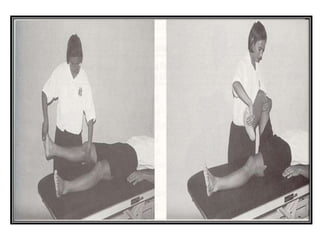
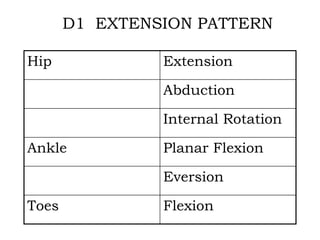
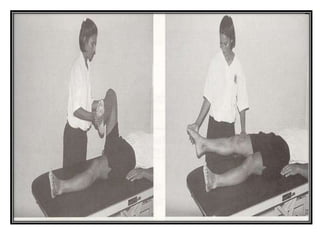
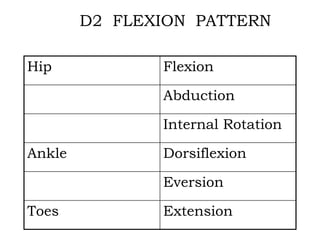
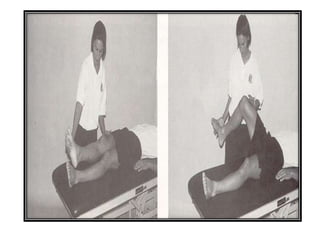
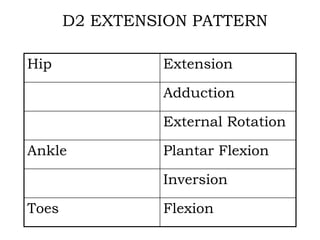
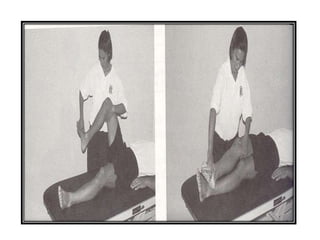
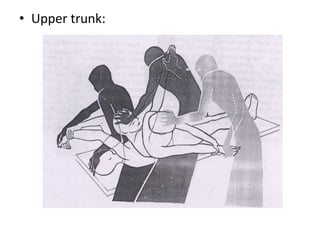
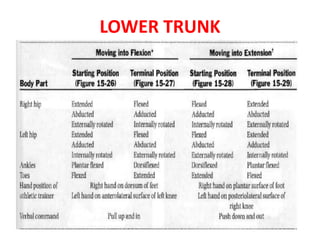
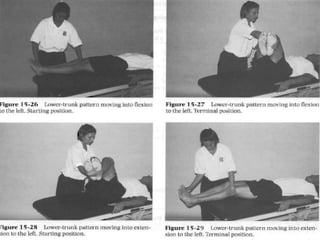
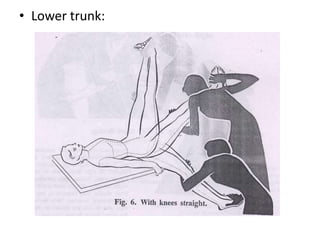
Proprioceptive neuromuscular facilitation (PNF) is an exercise technique based on principles of neurophysiology and functional anatomy. It uses patterns of diagonal movements combining flexion, extension, abduction, adduction, and rotation. The 9 principles of PNF include resistance, stretch, timing, and verbal commands. PNF techniques like repeated contractions and hold-relax are used to improve areas like strength, flexibility, and motor control by facilitating agonist and antagonist muscle groups. PNF patterns involve multi-joint diagonal movements of the upper and lower extremities.