Downloaded 254 times




![REFERENCES
Butler D, Mobilisation of the nervous system. New York: Churchill Livingstone; 1991
Haftek J. Stretch injury of peripheral nerve: acute effects of stretching on rabbit nerve. Joumal of
Bone and Joint Surgery 1970; 52B; 354-365.
Lundborg G. Ischemic nerve injury: experimental studies on intraneural microvascular
pathophysiology and nerve function in a limb subjected to temporary circulatory arrest.
Scandinayian Joumal of Plastic and Reconstructive Surgery 1970; 6: 1-113.
Selander D, Mansson L G, Karlsson L, i wsp. Adrenergetic [RACZEJ adrenergic] vasoconstriction in
peripheral nerves in the rabbit. Anesthesiology 1985; 62; 6-10.
Gilliatt R W. Physical injury to peripheral nerves: physiologic and electrodiagnostic aspects. Mayo
Clinic Proceedings 1981; 56; 361-370.
Triano J J, Luttges MW. Nerve irritation: a possible model of sciatic neuritis. Spine 1982; 7; 129-136.
Rydevik B, Brown M D, Lundborg G. Pathoanatomy and pathophysiology of nerve root
compression. Spine 1984; 9: 7-15.](https://image.slidesharecdn.com/neurodynamics-151220194109/85/Neurodynamics-38-320.jpg)

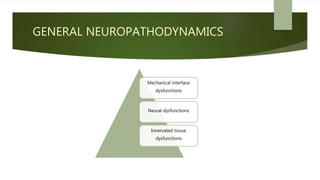
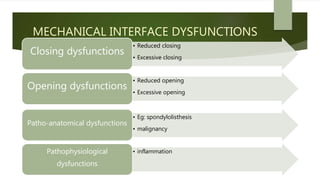
The document discusses neuropathodynamics and neuromobilization techniques. It covers: - Flexion and extension of the spine and their effects on neural tissues, producing tension and sliding. - Lateral flexion and its effects of increasing tension on the convex side and reducing tension on the concave side. - Various mechanical interface and neural dysfunctions that can occur. - Objectives, clinical tests, and techniques used in neuromobilization to restore normal neuromechanical function. - Contraindications for neuromobilization include acute injuries or infections of the nervous system. - Different levels of neurodynamic testing based on symptoms and neurological status.