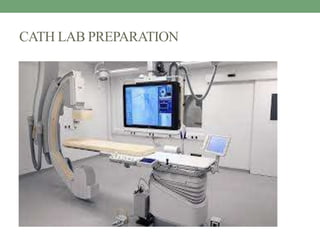
Cath lab preparation involves sterile setup of equipment and supplies. The sterile field must be carefully maintained to prevent infection. Patients are prepared by explaining procedures, identifying them, obtaining consent, and checking vitals. Emergency drugs and supplies are readied. Proper sterile technique includes scrubbing, gowning, gloving and draping. Procedures like angiograms, angioplasty, stent placement and temporary or permanent pacemakers require specific tray setup and patient preparation. Post-procedure care includes sheath removal, monitoring for bleeding, and discharge education on wound care and activity restrictions.








































![Con…
Trolley preparation:
• same to CAG +
• Pacing catheter
• Pacemaker generator [keep ready outside]
• Suturing materials to fix the pacing wire.
Preparing of the patient:
• same to CAG](https://image.slidesharecdn.com/pptcathlabpreparation11-230424194737-d96e8064/85/PPt-Cath-lab-preparation-1-1-pptx-56-320.jpg)















![Sheath removal
A tray containing:
• Inj. Atropine [1 ampule loaded in 2cc syringe]
• Sterile gauze pieces, IV set, IV F-NS
• Betadine solution
• Plaster
• Sterile gloves](https://image.slidesharecdn.com/pptcathlabpreparation11-230424194737-d96e8064/85/PPt-Cath-lab-preparation-1-1-pptx-74-320.jpg)
![Con…
• Feel the femoral pulse by using middle finger and index finger.
[1-2 inch above the puncture site]
• Ask the patient to hold the breath.
• Slowly loose the finger and remove the sheath.
• As soon as the sheath comes out, allow the 1-2 drop of blood to
flow out.](https://image.slidesharecdn.com/pptcathlabpreparation11-230424194737-d96e8064/85/PPt-Cath-lab-preparation-1-1-pptx-76-320.jpg)

![Con…
• Check the distal pulse to confirm flow.
• Once hemostasis is established by manual compression,
• Mechanical device should not be used [sand bags, clamps].](https://image.slidesharecdn.com/pptcathlabpreparation11-230424194737-d96e8064/85/PPt-Cath-lab-preparation-1-1-pptx-78-320.jpg)






























































































