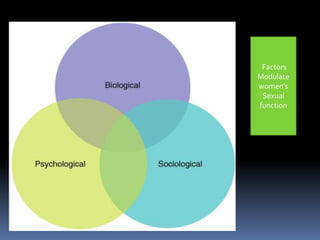
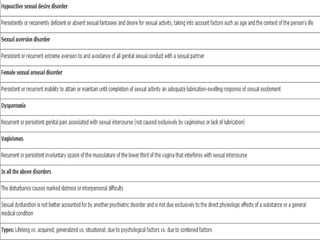
This document discusses sexuality and sexual dysfunction. It covers several topics including the definition of sexuality, factors that influence women's sexual function, models of the female sexual response cycle, physiology of sexual desire and arousal, and risk factors and causes of sexual dysfunction. It also discusses how various medical conditions, drugs, and obstetrics-gynecology problems can influence sexual function.