Scenario 1
A 32year old lady P2 c/o spotting in between her periods, post coital
bleeding with regular periods which lasts for 4-6 days, mild dysmenorrhoea,
no dyspareunia. There is no significant medical history. There was a h/o STI in
past which was treated successfully and she is in stable relationship for 5
years. She takes CHC.
4.
Scenario 2
A48 year old lady P2 with a h/o normal and regular periods in past. She
is c/o irregular periods with prolonged bleeding pattern lasting for 5-9
days for 6-8 months . No post coital or intermenstrual bleeding. She had
an USS done recently showing ET 2.5 mm with normal ovaries. Her recent
blood tests are normal. She uses condoms as contraception.
5.
Scenario 3
4.A 25-year-old woman who has been using the progestogen-only
implant presents with irregular bleeding since starting 7 months ago and
would like treatment or for it to be removed. She has no significant
medical history. After consideration and exclusion of other factors, what
is the appropriate treatment to offer her?
6.
Scenario 4
3.A 37-year-old woman who has had the levonorgestrel-releasing
intrauterine system (LNG-IUS) for 9 months complains about the irregular
spotting she has always experienced with this method. She wishes to
control the bleeding while on holiday. She has no contraindications to
hormonal contraceptives.
7.
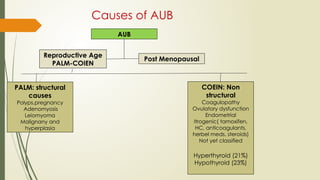
Causes of AUB
AUB
ReproductiveAge
PALM-COIEN
Post Menopausal
PALM: structural
causes
Polyps,pregnancy
Adenomyosis
Leiomyoma
Malignany and
hyperplasia
COEIN: Non
structural
Coagulopathy
Ovulatory dysfunction
Endometrial
Itrogenic( tamoxifen,
HC, anticoagulants,
herbel meds, steroids)
Not yet classified
Hyperthyroid (21%)
Hypothyroid (23%)
8.
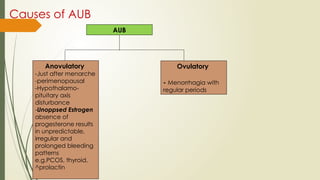
Causes of AUB
AUB
Anovulatory
-Justafter menarche
-perimenopausal
-Hypothalamo-
pituitary axis
disturbance
-Unoppsed Estrogen
absence of
progesterone results
in unpredictable,
irregular and
prolonged bleeding
patterns
e.g.PCOS, thyroid,
^prolactin
Ovulatory
- Menorrhagia with
regular periods
9.
How to approach
History:
age, Menstrual Hx, Sexual Hx, Obstetric/ Gynae Hx
Past medical Hx
Drug Hx
Family Hx
Examination: systemic illness, galactorrhoea, A Nigricans, hirsuitism,
Acne, Abdo, PS, PV
Investigations: Exclude pregnancy, Swabs for STI, Check recent Cx screening
result, Blood test( FBC, Clotting, TFT, LFTs), USS pelvis
Treatment: Treat the cause
10.
Treatment of Anovulatorybleeding
Progestogens like Nor-Ethisterone or medroxyprogesterone
To arrest the heavy bleeding
Then cyclically
COC pills for 3-6 months
11.
Treatment of heavymenstrual
bleeding (Menorrhagia)
If women is not wishing for contraception or while waiting for the Investigations/if
fibroid is less than 3 cm
Mefanemic acid with Tranexamic acid is the 1st
choice
If Long term contraception is acceptable then
LNG-IUS is the 1st
choice
2nd
Choice
COC that reduces dysmennorhoea and regulate cycles
3rd
Choice
Nor-ethisterone day 5-26 ( not effective contraception, but may inhibit ovulation)or
Depo- provera 12 weekly
GNRH analougues Not recommended in PC, but a good option in SC
12.
Treatment of Menorrhagia
Ifinitial 1st
line Rx fails then combine
Tranexamic acid + Nsaids (dysmenorrhoea)
Nsaids + COCpills
To arrest heavy bleeding
NEST 5mg- 10mg tds for 10 days ( stops bleeding with in 1-3 days, with drawl bleed
occurs 2-4 d after stopping Rx)
REFERRALS:
Alarm symptoms
QOL is negatively affected by menorrhagia
Women wishes to have surgery
Fe deficiency anaemia that fails to respond to pharmaceutical treatment
13.
Problematic bleeding withhormonal
contraception
It is challenging. For many women it is due to the contraceptive method itself
Women may consider that the contraceptive and non-contraceptive benefits of
a method outweigh the inconvenience of unpredictable bleeding.
Assessment should be by
● Clinical history
● Exclude STI - perform speculum exam and take swabs at least for chlamydia
● Check cervical screening history
● Consider the need for a pregnancy test
● Exclude underlying pathology
14.
Medical Therapy optionsfor women using
hormonal contraception with problematic Bleeding
CHC users Reassurance for 1st 3 M , increase EE up to max 35micrograms
POP users may try a different POP, Estrogen supplementation or
tranexamic acid
PO implants, injectibles and IUS EE 30-35 micr with LNG/ norethisterone or
mefanemic acid 500mg tds with tranexamic acid 1gm qds as s short term
therapy.
Scenario 5
A55 year old lady with an LMP 5 years ago presented with vaginal
bleeding off and on. She is sexually active. She denies any medical history
and does not take any OTC medications. O/E BP 142/88, BMI of 35, fresh
bleeding in the vagina with a small blood clot on her right labia. Cervix
looks healthy. Bimanual examination is satisfactory.
How will you proceed?
17.
History
When?
Nature,precipitating factors like SI, Trauma
Discharge
HRT, tamoxifen, Anticoagulants
Any recent unintentional weight loss, fever, abdo pain, personal and family h/o
endometrial, breast, ovarian / colon cancers, (LYNCH II) bladder bowel change
Parity
Age of menarche and menopause
Smoking HTN, DM
Last smear result
18.
Examination
Vital signs
BMI
Signs of anaemia
Abdominal examination to assess the size, Contour, tenderness of uterus,
visceromegaly, ascites.
Speculum examination – see vulva, vagina, signs of atrophy, bleeding,
growths on vaginal wall/ cervix, abnormal discharge
Bimanual exam to look for size of uterus, mobility, fullness of adnexa and
tenderness.
If suspected endometrial cause of bleeding, perform the pipelle biopsy and
refer as 2WW ref to gynaecology.
19.
Atrophic Vaginitis
Presentswith soreness and dryness of vagina, vaginal bleeding, supf dyspareunia,
dysuria, recurrent UTI and vaginal discharge.
Thinning of the vulval and vaginal epithelium
Loss of glycogen
Fall in acidity
Absence of protective lactobacilli
Estriol creams/ pessaries daily for 2 weeks then twice weekly for 3 months.(Ovestin,
Vagifem, Orthogynest, Premique, Prempak)
No evidence that topical Estrogens causes endometrial proliferation after 6-24 m of
use therefore no need to prescribe systemic progestogens.
Vaginal lubricants can be use with or with out local Estrogen treatment.
20.
PMB with HRT
Unscheduled Vaginal bleeding is a common adverse effect of HRT in first
3m of treatment.
CCHRT- Commonly produces irregular breakthrough bleeding in first 4-6 m.
Bleeding beyond 6m or after the spell of amenorrhoea requires further
investigations. Once risk of malignancy is excluded then try low dose
Estrogen or ^ progesterone regimen.
Sequential HRT should produce regular predictable bleeding starting
towards or soon after the end of progesterone phase. Increasing the
duration, dose or type of progestogen is recommended.