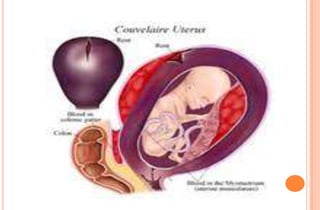
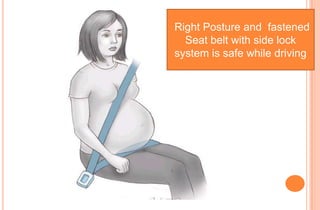
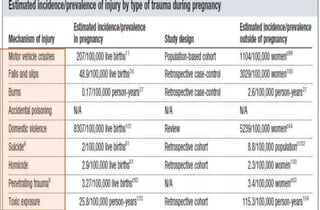
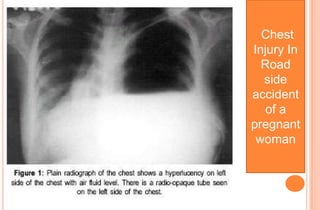
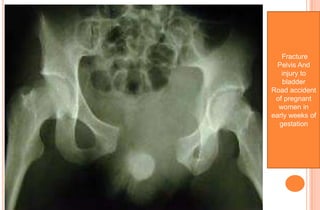
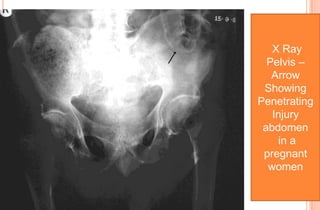
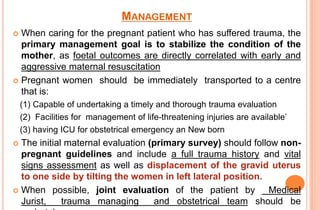
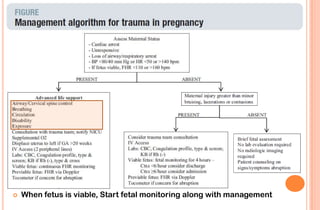
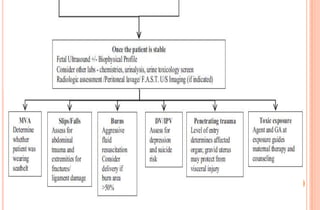
This document discusses trauma during pregnancy, its types and management. It begins by describing common causes of trauma like motor vehicle accidents, falls, burns and domestic violence. It then discusses complications of trauma during specific periods of pregnancy. Trauma increases risks of abortion, preterm birth, placental abruption and fetal distress. Motor vehicle crashes are a leading cause while falls commonly occur at home. Management involves stabilizing the mother through aggressive resuscitation since fetal outcomes depend on maternal condition. Investigations may be conducted after weighing risks to fetus from radiation exposure.