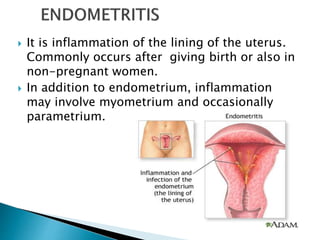
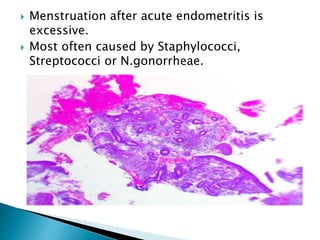
Endometritis is the inflammation of the endometrium, the uterine lining, often caused by infections such as chlamydia and gonorrhea, especially following childbirth or medical procedures. Symptoms include dysmenorrhea, abnormal vaginal discharge, fever, and lower abdominal pain, with acute and chronic forms presenting with different histological features. Chronic endometritis may be associated with underlying cancers of the cervix or endometrium.