This document summarizes the evaluation and treatment of shoulder instability. It describes the history, physical exam maneuvers like the anterior apprehension test, imaging studies including MRI and CT, and surgical procedures to address anterior and posterior instability like Bankart repair, Latarjet procedure, and remplissage. Key points are identifying the direction and chronicity of instability, assessing for bone defects, and selecting the appropriate surgical techniques to restore stability while maintaining function.

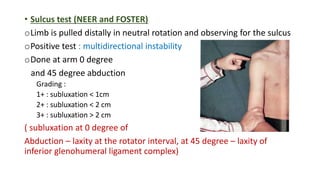
![• Frequency of dislocation
• Ease with which relocation occurs
• Precipitating factors [like seizure]
• Generalized ligament laxity: dislocation reduces by the patient himself
• h/o Dislocations during sleep or with the arm in an overhead position
• h/o having a dead arm](https://image.slidesharecdn.com/shoulderinstability-230607165557-e9ec3359/85/SHOULDER-INSTABILITY-pptx-3-320.jpg)