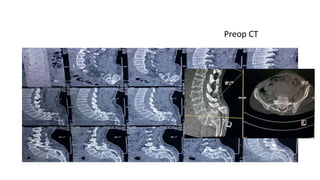
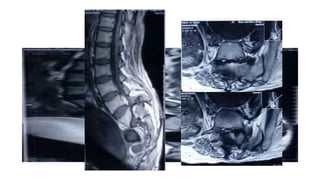
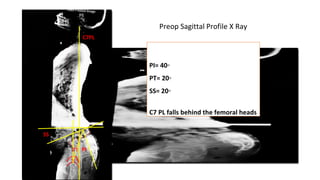
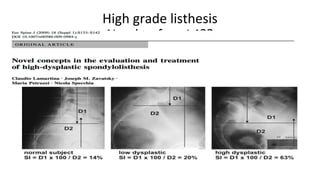
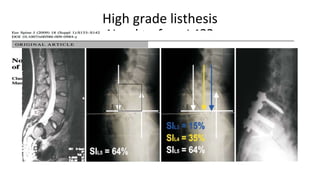
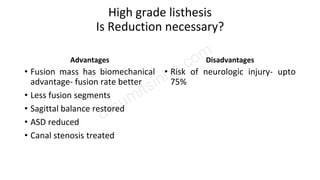
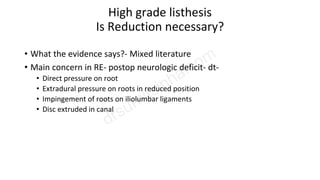
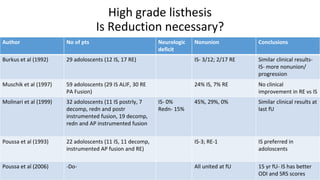
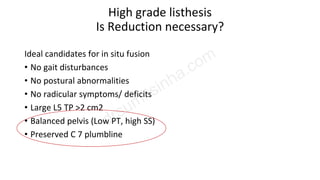
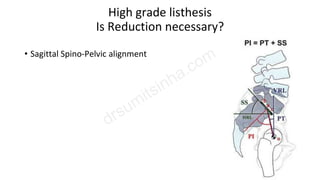
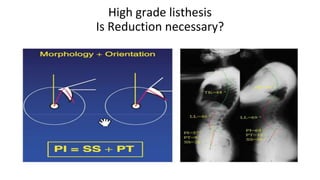
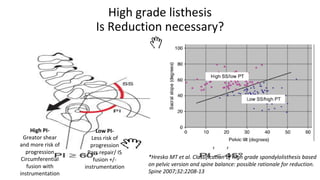
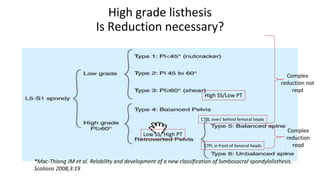
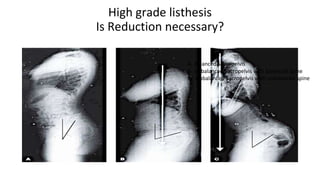
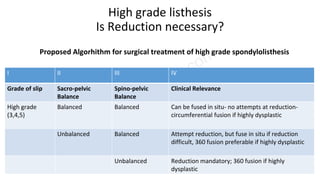
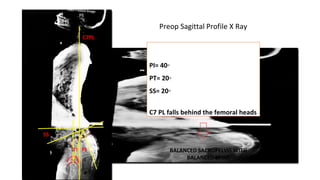
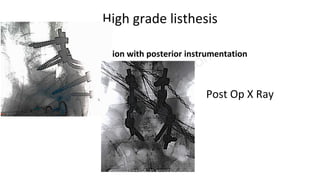
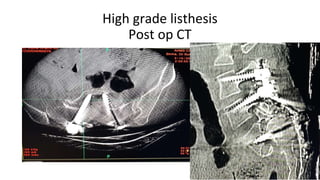
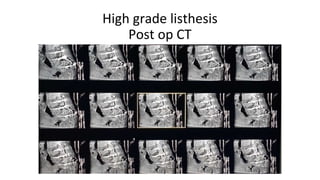
This document discusses the treatment of high grade spondylolisthesis. It considers whether reduction is necessary or if in situ fusion is preferable. Reduction carries risks of neurologic injury but may provide biomechanical advantages. The ideal treatment depends on factors like sagittal and pelvic balance, the presence of symptoms, and L5 transverse process size. For balanced sacropelvises with balanced spines, in situ fusion without reduction is often sufficient. Unbalanced cases may require reduction or circumferential fusion. The case presented involved a balanced patient who was treated successfully with in situ fusion using posterior instrumentation alone.