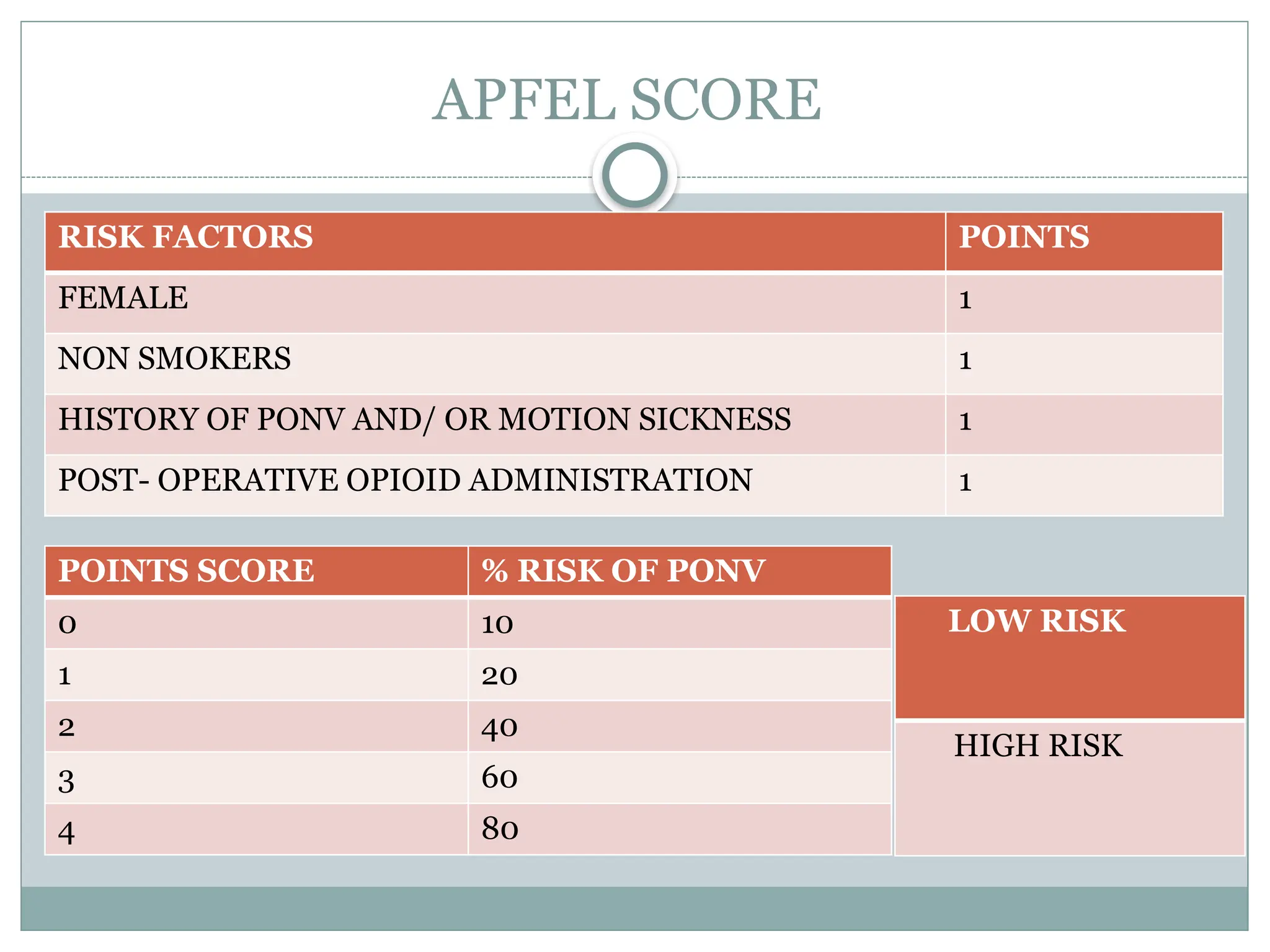
Postoperative nausea and vomiting (PONV) are common complications following anesthesia and surgery, with a nausea incidence of 22% to 38% and vomiting 12% to 26%. Factors contributing to PONV include patient characteristics (like young age and female gender), type of anesthesia, and specific surgical procedures. Various prophylactic treatments such as 5-HT3 receptor antagonists and corticosteroids can be effective in reducing the risk of PONV, with ondansetron and dexamethasone being among the most commonly recommended medications.