Post operative nauseaand
vomiting
Presenter - Dr Tanmay Patil
Moderator- Dr Ravi Khandelwal
2.
DEFINITIONS
VOMITING :Forceful expulsion of gastric contents
through mouth and nose
NAUSEA : Sensation of unease and discomfort in stomach
with urge to vomit
RETCHING : similar to vomiting with the exception that
no gastric content enters the pharynx.
3.
PONV istypically used to describe nausea and
vomiting or retching in post anaesthesia care unit
or in immediate 24 postoperative hrs.
PONV can delay recovery room discharge or may
required unanticipated hospital stay.
These can leads to rare but serious conditions like
wound dehiscence ,esophageal rupture,
aspiration, subcutaneous emphysema or
pneumothorax .
4.
Introduction
Without aprophylaxis, Postoperative nausea and
vomiting (PONV) occurs in approximately 20% to 30% of
general surgical population and up to 70-80% in patients
with predisposing risk factors.
PONV is second most common (pain is most common)
complaint reported after surgery. As anesthetic
duration increases, so too, does PONV risk .
When the risk is sufficiently great, prophylactic anti
emetic medications are administered and strategies to
reduce its incidence are initiated.
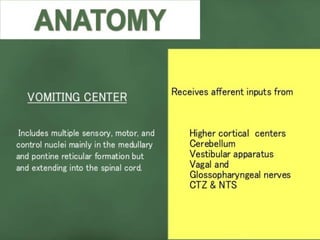
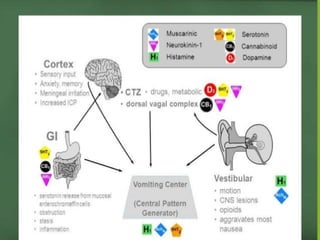
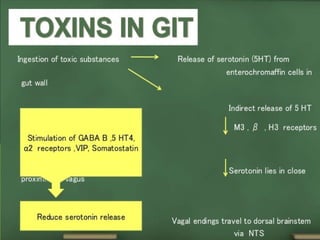
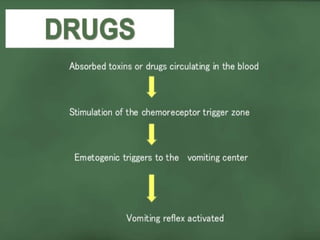
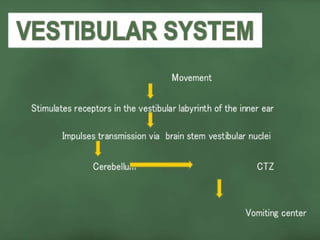
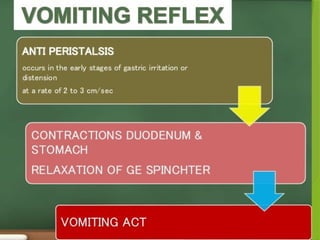
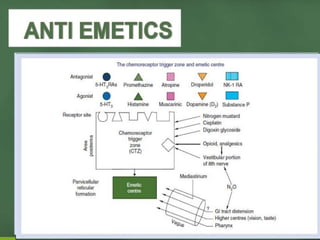
Nausea and vomiting may be induced through various
pathways , which finally stimulate vomiting center in
brain stem.
11.
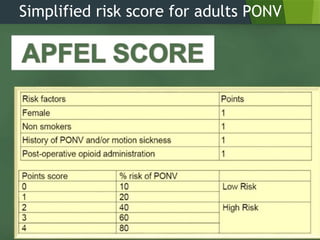
Risk factors forpostoperative
nausea and vomiting (PONV)
(1)Patient-specific risk factors:
-Female gender
-Nonsmoking status
-History of PONV/motion sickness
(2)Anesthetic risk factors:
-Use of volatile anesthetics
-Use of nitrous oxide
-Use of intraoperative and postoperative opioids
- Duration of anaesthesia.
(3)Surgical risk factors:
-Duration of surgery (each 30-min increase in duration
increases PONV risk by 60%, so that a baseline risk of
10% is increased by 16% after 30 min)
-Type of surgery -Laproscopic surgeries, ENT
surgeries,cholecystectomy,strabismus surgery.
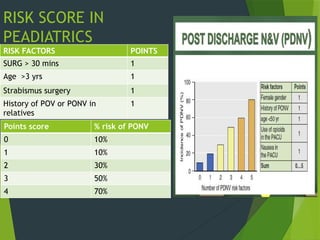
RISK SCORE IN
PEADIATRICS
RISKFACTORS POINTS
SURG > 30 mins 1
Age >3 yrs 1
Strabismus surgery 1
History of POV or PONV in
relatives
1
Points score % risk of PONV
0 10%
1 10%
2 30%
3 50%
4 70%
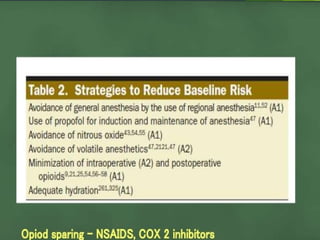
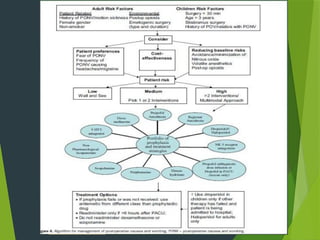
Combination and multimodal
therapy
None of the currently available antiemetic is capable of
completely eliminating the incidence of PONV. The patients
baseline risk is main determent of the effectiveness of
antiemetic interventions.
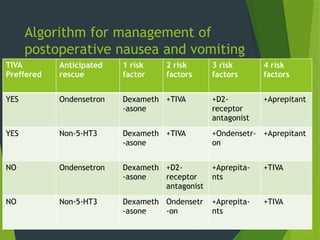
Therefore, prophylaxis is rarely justified in patients at low
risk, a single antiemetic is likely to be reasonable for
patients with a moderate risk, and patients at high risk are
likely to benefit from combination treatment.
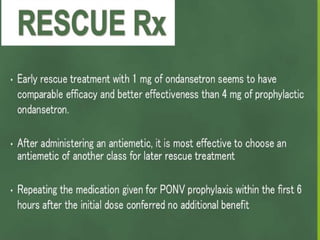
After administering an antiemetic, it is more effective to
choose an antiemetic of another class for later rescue
treatment.












































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)








