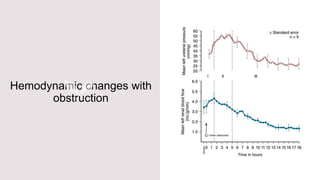
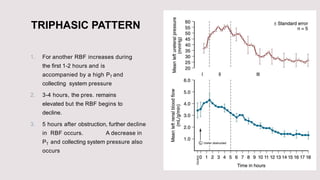
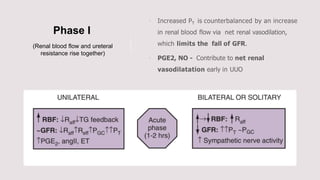
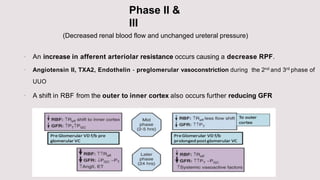
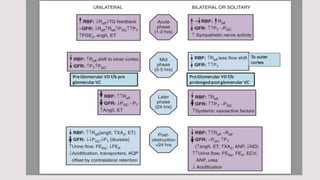
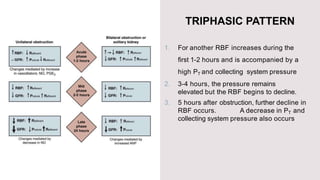
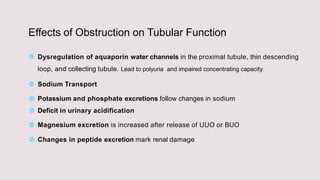
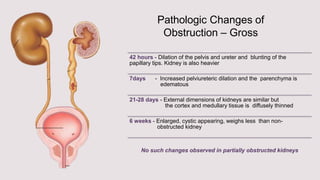
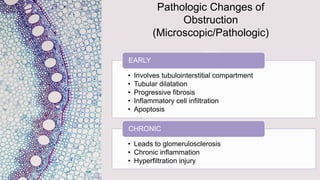
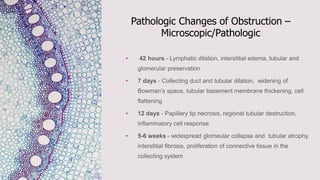
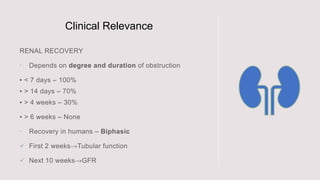
This document discusses the pathophysiology of unilateral ureteric obstruction. It describes three phases that occur with obstruction: 1) renal blood flow increases initially along with pressure, 2) pressure remains elevated but blood flow declines, 3) further declines in blood flow and decreases in pressure. The obstruction causes vasoconstriction that reduces blood flow and glomerular filtration rate over time. Microscopic changes include tubular dilation, fibrosis, inflammation and apoptosis leading to glomerulosclerosis and chronic inflammation. Clinical relevance includes risk of hypertension, proteinuria and declining renal function with loss of nephrons if obstruction is not relieved.