This document discusses transrectal ultrasound (TRUS)-guided prostate biopsy. It begins with an introduction to declining prostate cancer mortality due to early detection programs using prostate-specific antigen (PSA) testing and TRUS-guided biopsy. It then covers the ultrasonographic anatomy of the prostate visible on TRUS, different TRUS biopsy techniques, indications for biopsy, and advanced ultrasound techniques like color and power Doppler that can help identify areas of neovascularity suspicious for cancer. The document provides a comprehensive overview of how TRUS is used to image the prostate and guide systematic biopsies for prostate cancer detection and diagnosis.












































![Powerpoint Templates
Page 50
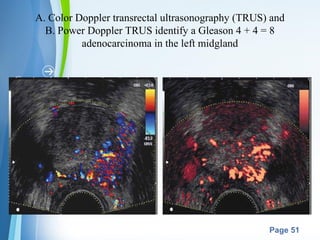
POWER DOPPLER IMAGING
(enhanced color Doppler, color
amplitude imaging [CAI], or color
angiography)
• uses amplitude shift to detect flow in
a velocity and directionally
independent manner.
• Advantages: ability to detect slower
flow and to have less reliance on the
Doppler angle, making it more
suitable for detection of prostate
cancer neovascularity.](https://image.slidesharecdn.com/trusbiopsyprostate-150621060724-lva1-app6892/85/Trus-biopsy-prostate-50-320.jpg)