
Downloaded 19 times



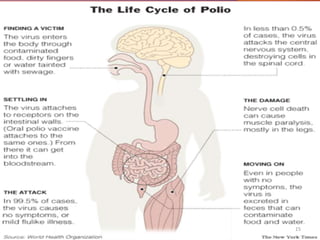


Poliomyelitis, commonly called polio, is caused by the poliovirus. It spreads through fecal-oral transmission and can cause paralysis in rare cases. Children under 5 are most at risk. While outbreaks were once common, vaccination efforts have led to polio being eradicated in most countries. Both inactivated and live attenuated polio vaccines provide effective immunity, though the live version has advantages of lower cost and stronger intestinal immunity. With continued vaccination, polio can be eliminated worldwide.

















































































