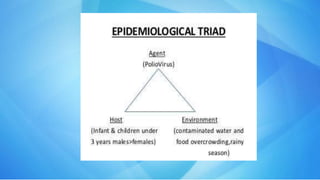
Poliomyelitis is an infectious disease caused by the poliovirus that infects the brain and spinal cord, potentially causing paralysis. It is most commonly spread through contaminated fecal matter entering the mouth. While it can affect people of any age, children are most susceptible. Prevention through vaccination has been very effective, with India eliminating the disease through widespread immunization programs. Surveillance of cases of paralysis and environmental sampling helps monitor transmission and outbreaks.