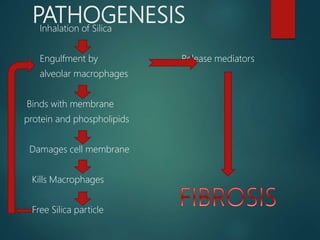
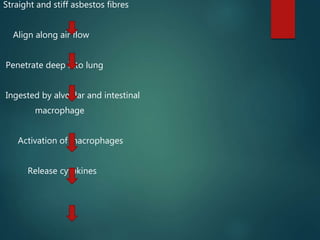
Pneumoconiosis is a lung disease caused by inhaling particles like coal dust, silica, asbestos, and other organic and inorganic materials. Important types include coal worker's pneumoconiosis, silicosis, and asbestosis. Silicosis results from inhaling silica, which is engulfed by macrophages but kills them, releasing free silica and perpetuating a cycle of lung injury and fibrosis. Asbestosis is caused by inhaling asbestos fibers, which can penetrate deep into the lungs and cause fibrosis when macrophages that engulf them release cytokines. Both silicosis and asbestosis can lead to complications like lung dysfunction, cor pulmonale, and an increased risk of cancer over time