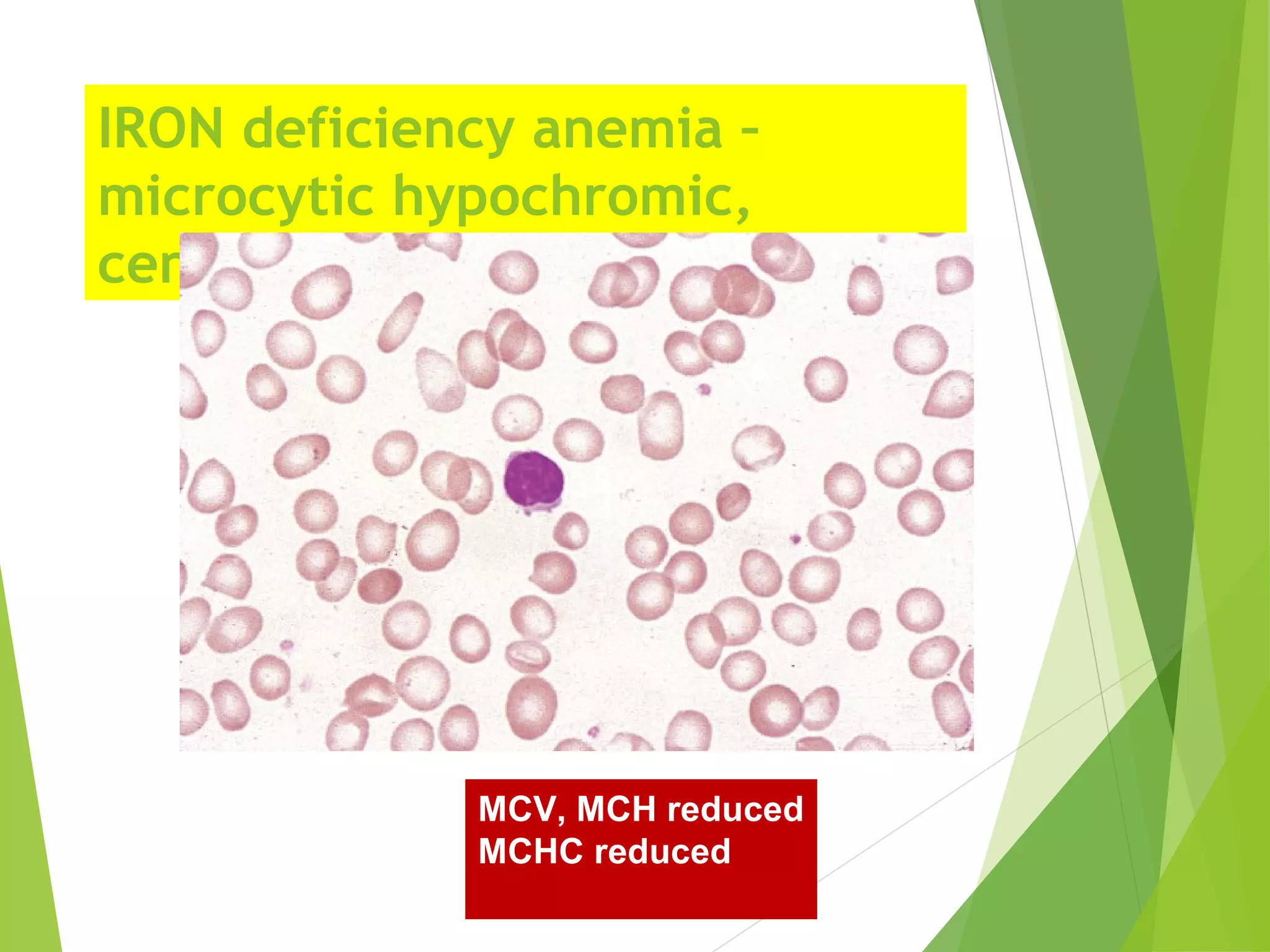
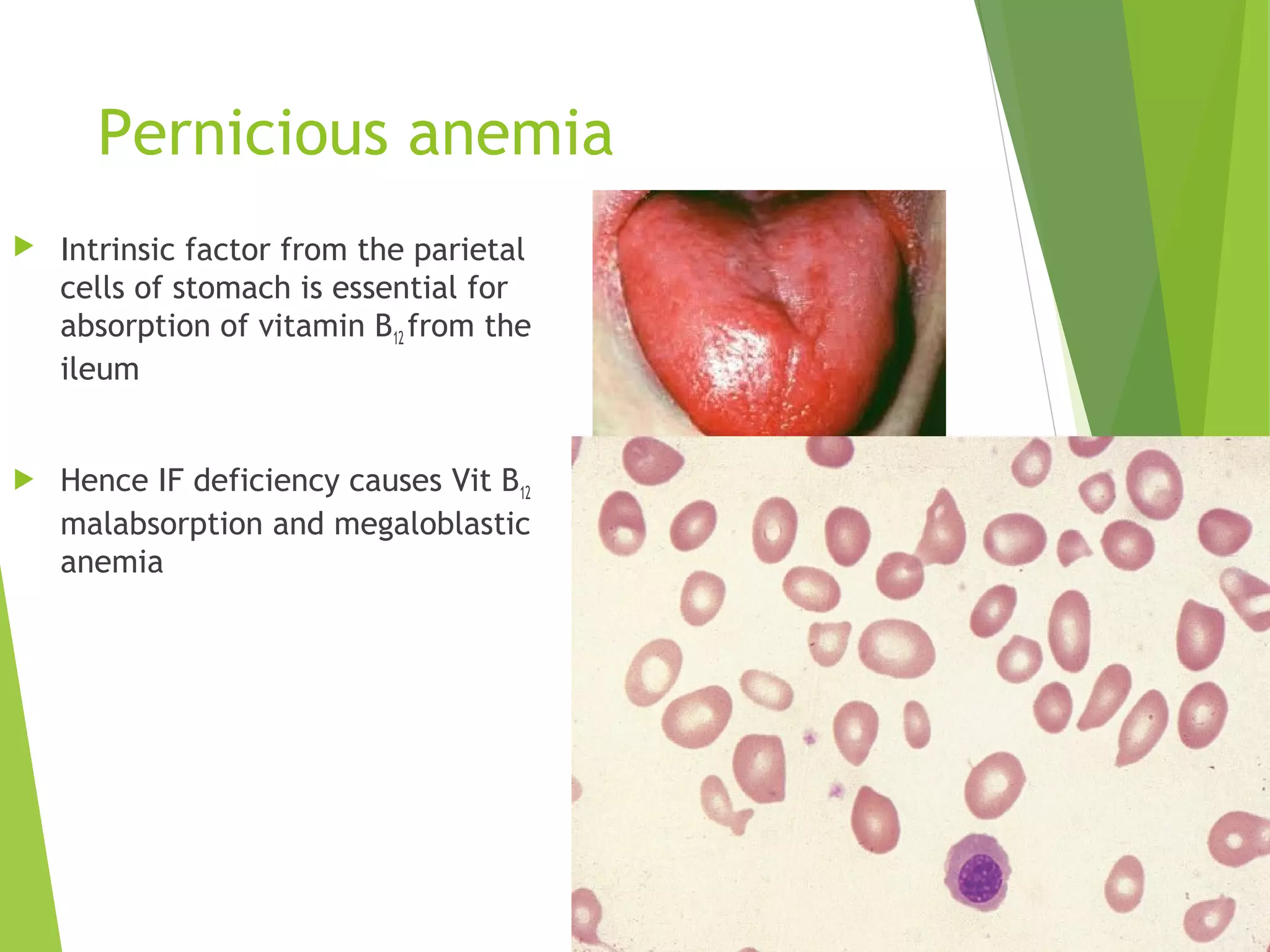
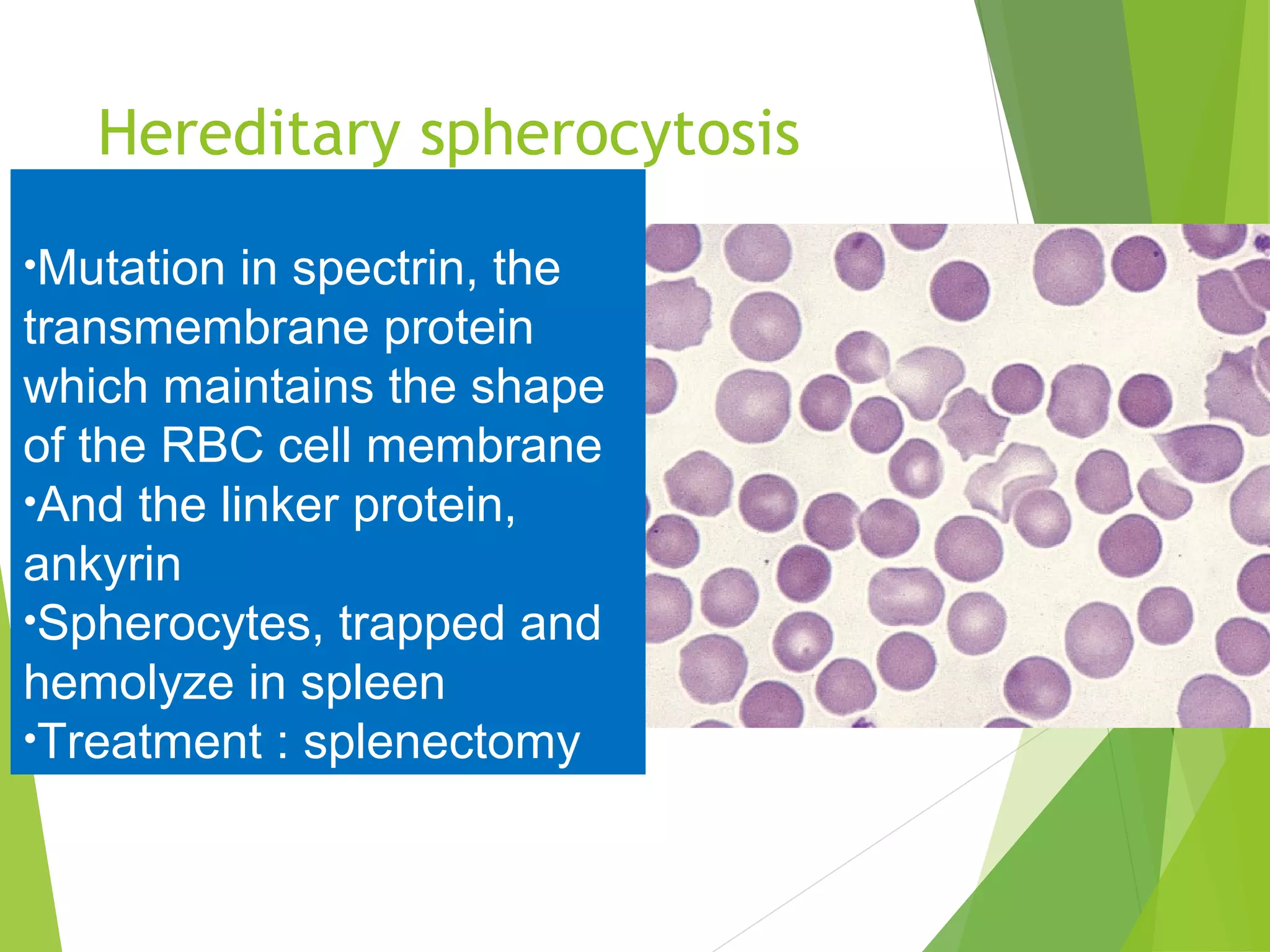
This document discusses anemia, including its definition, classification, causes, symptoms, diagnostic tests, and treatment. It defines anemia as a reduction in red blood cells or hemoglobin. Anemia is classified morphologically based on cell size and shape or etiologically based on cause. Common causes include iron deficiency, megaloblastic anemia related to B12 or folate deficiency, sickle cell anemia, thalassemia, and anemia of chronic disease. Diagnostic tests include complete blood count, blood smear, and iron/B12/folate levels. Treatment depends on the underlying cause but may include oral/IV iron, B12/folate supplements, blood transfusions, or splen


























































![BLOOD_DISORDERS-2[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/blooddisorders-21-230610142333-f4472c75-thumbnail.jpg?width=640&height=640&fit=bounds)




















































