Occupational lung disease can result from inhaling dusts, fumes or other substances on the job. Common examples include pneumoconiosis caused by inhaling mineral dusts like coal, silica or asbestos. Coal workers' pneumoconiosis and silicosis develop due to deposition of dust deep in the lungs, causing inflammation and fibrosis over time. Asbestosis and certain cancers are associated with asbestos exposure. Chest x-rays and pulmonary function tests can help diagnose these conditions. Prevention involves eliminating dust exposure through measures like ventilation and use of protective masks.















![ASBESTOSIS
MALIGNANCY
1.Malignant mesothelioma
2. Bronchogenic carcinoma
PLEURAL
1.Plaque
2.Effusion
3.Thickening
4.Calcification
PARENCHYMAL DISEASES
1.Asbestosis [parenchymal fibrosis
caused by asbestos inhalation]
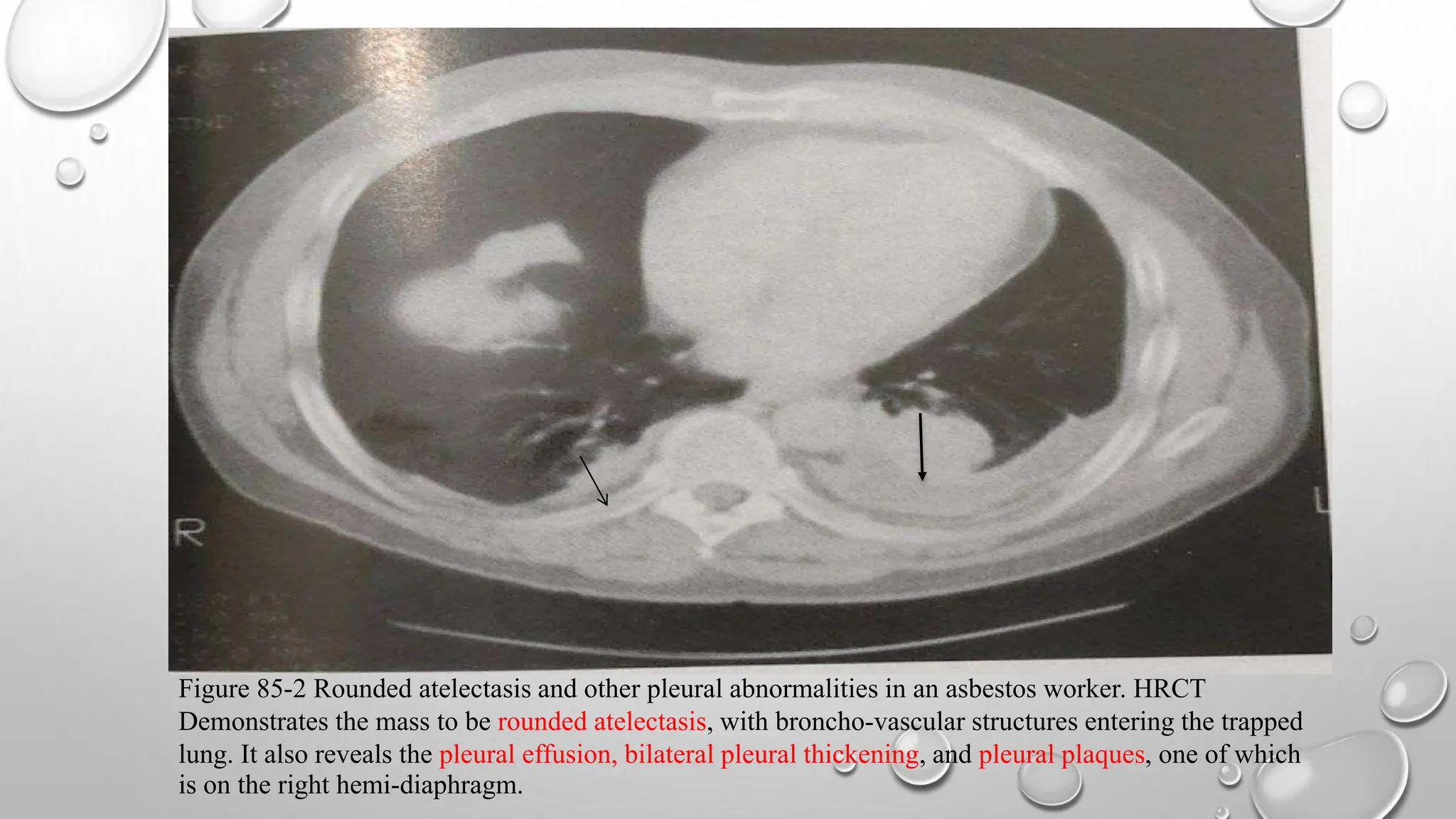
2.Rounded atelectasis
3.Benign fibrotic masses
4.Transpulmonary bands
BENIGN](https://image.slidesharecdn.com/occupationallungdisorders1-240307063245-dbbd7755/75/OCCUPATIONAL-LUNG-DISORDERS-by-postgraduate-students-pptx-17-2048.jpg)