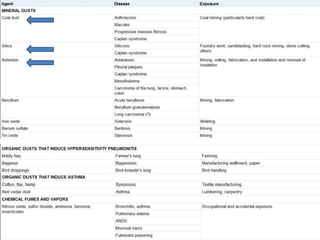
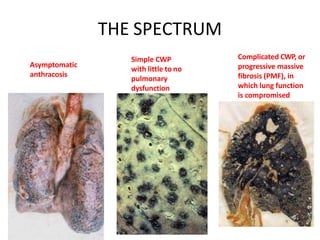
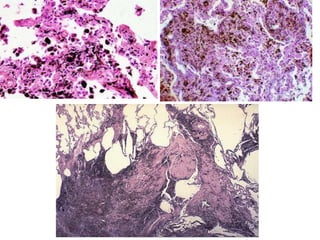
1) Pneumoconiosis refers to lung diseases caused by inhaling mineral dust including coal workers' pneumoconiosis and silicosis.
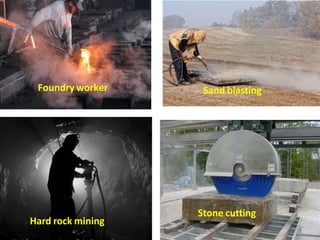
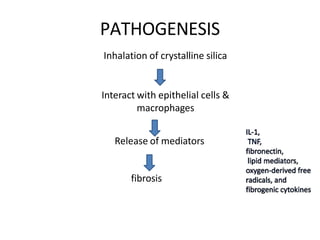
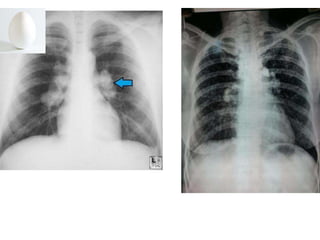
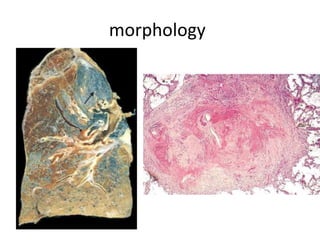
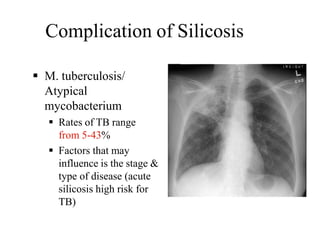
2) Silicosis results from inhaling crystalline silica and presents as nodular lesions in the lungs. High risk jobs include mining, sandblasting, and foundry work.
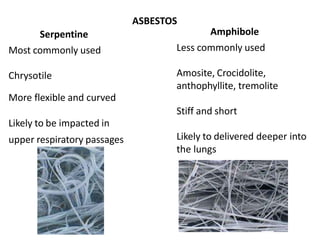
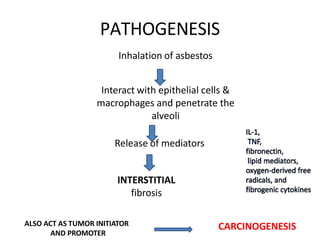
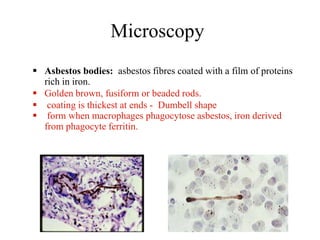
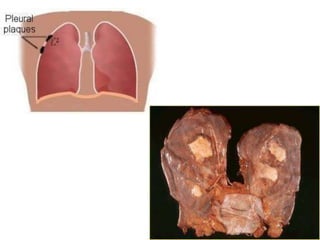
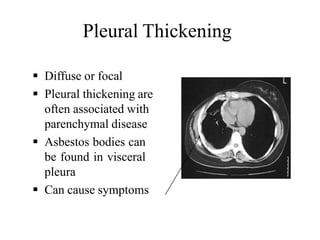
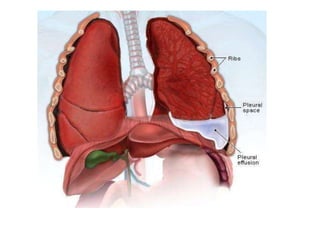
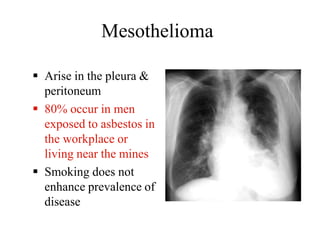
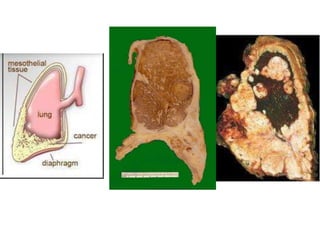
3) Asbestosis is pulmonary fibrosis caused by inhaling asbestos fibers which can lead to complications like mesothelioma and lung cancer decades later. Asbestos was commonly used in insulation and construction.