When assessingan abdominal x-ray
1. Check for the patient details
2. Check which projection has been
used
3. Check and ensure you can see the
whole abdomen
4. Systematically review bowel gas ,soft
tissues ,bones and abnormal
calcifications
Normal stomach maybe visible if it contains
air and is visible in the left upper quadrant
of the abdomen .The lowest part of the
stomach crosses the midline
5.
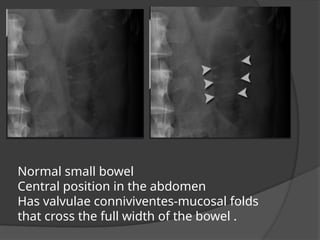
Normal small bowel
Centralposition in the abdomen
Has valvulae conniviventes-mucosal folds
that cross the full width of the bowel .
6.
Normal large bowel
Peripheralposition in the abdomen (the transverse
and sigmoid colon occupy very variable positions)
Haustra
Contains faeces
7.
Liver on abdominalX-ray
The liver lies in the right upper quadrant (RUQ) and is seen as a bland area of grey
on an abdominal X-ray.
The superior edge of the liver forms the right hemi-diaphragm contour
In this patient the breast shadow (red line) overlies the liver, and markings of the
right lung are visible behind the liver.
The gallbladder is only rarely visible on an abdominal X-ray. Its position is very
variable. This patient has had a cholecystectomy. The clips mark the previous
location of the gallbladder.
8.
Lung bases onabdominal X-ray
The lung bases, which pass behind the liver and diaphragm in the posterior
sulcus of the thorax, may be visible on some abdominal X-rays.
It is worth checking the lung bases as some patients with lung pathology
present with abdominal symptoms.
If there is consolidation suspected from the abdominal X-ray then a review
of the patient's respiratory system is necessary.
Costophrenic angle .
9.
Psoas edges onabdominal X-ray
The psoas muscles arise from the transverse processes of the lumbar vertebrae
(arrowheads) and combine with the iliacus muscles. Together these powerful muscles
form the iliopsoas tendon, which attaches to the lesser trochanter of the femur (asterisk).
The iliopsoas muscles are the flexors of the hip.
An abdominal X-ray often demonstrates the lateral edge of the psoas muscles as a near
straight line. The iliacus muscles are not visible, as they lie over the iliac bones of the
pelvis.
10.
Kidneys on abdominalX-ray
Natural contrast between the kidneys and the low density retroperitoneal
fat that surrounds them means they are often visible on an X-ray of the
abdomen.
They lie at the level of T12-L3 and lateral to the psoas muscles. The right
kidney is usually slightly lower than the left due to the position of the liver.
11.
Spleen on abdominalX-ray
The spleen lies in the left upper quadrant
immediately superior to the left kidney.
12.
Bladder abdominal X-ray
Thebladder has variable appearance depending
on how full it is. It has the same density as other
soft tissue structures, due to its water content.
13.
Normal bones onabdominal X-ray
The lower ribs, lumbar vertebrae and sacrum are highlighted.
Bones can be used as landmarks for invisible soft tissue structures. Note
the transverse processes of the lumbar vertebrae act as landmarks for the
course of the ureters (arrowheads). The vesico-ureteric junctions
(asterisks) are located at the level of the ischial spines (arrows).
14.
Normal bones onabdominal X-ray
The sacrum, coccyx, pelvic bones and proximal
femora are highlighted. The sacro-iliac joint is
formed by the overlapping of the sacrum and iliac
bones of the pelvis.
15.
None pathological densitiesand
artifacts
These densities cannot be explained
by anatomical structures are often
seen on abdominal X-rays
Added densities may be due to
artifact or calcified soft tissue
Calcification of soft tissues is not
always clinically significant
Differentiating pathological from
inconsequential calcification is not
always straightforward
16.
Navel jewellery artifact
Ideallyall jewellery that overlies
anatomically important structures should
be removed prior to acquiring an X-ray
17.
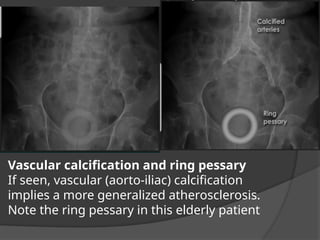
Vascular calcification andring pessary
If seen, vascular (aorto-iliac) calcification
implies a more generalized atherosclerosis.
Note the ring pessary in this elderly patient
18.
Calcified structures
There aremultiple incidental and asymptomatic calcified structures seen on this X-
ray.
The patient is recovering from an appendicectomy (note surgical clips).
Gallstones are seen only if calcified (20% are calcified). Although they may cause
symptoms they are usually asymptomatic. If gallstone disease is suspected
ultrasound examination is a more appropriate investigation.
Costochondral calcification, calcified mesenteric lymph nodes, and phleboliths
(calcified pelvic veins) are rarely clinically significant. Occasionally additional
investigations are required to differentiate them from pathological calcium. For
example phleboliths may be mistaken for ureteric calculi. Other investigations such
as intravenous urogram (IVU) or CT-KUB (CT Kidneys-Ureters_bladder) should only
19.
Residual contrast
The largeareas of very high density seen in the descending
colon and rectum are caused by residual contrast material in
this patient who had a Barium enema 10 days previously.
Also note costochondral calcification, and phleboliths.
Do not mistake the tips of the transverse processes for ureteric
calculi.
Bowel gas pattern
Note Any part of the bowel is visible if
it contains gas /air with in the lumen .
Gas is of low density and forms a
natural contrast against surrounding
denser soft tissues.
22.
Extraluminal air
• TYPES
–Pneumoperitoneum/free
air/intraperitoneal air
– Retroperitoneal
air(pneumoretroperitoneum)
– Air in the bowel wall (pneumatosis
intestinalis)
– Air in the biliary system (pneumobilia)
23.
Pneumoperitoneum /Free
gas
Isgas within the peritoneal cavity
often due to critical illness. There are
numerous causes and several mimics.
The most common cause of
Pneumoperitoneum is the disruption
of the wall of a hollow viscus. In
children, the causes are different
from the adult.
Causes of Pneumoperitoneum in
adults
perforated hollow viscus/Bowel
perforation
peptic ulcer disease
Ischemic bowel
bowel obstruction
necrotizing enter colitis
appendicitis
diverticulitis
malignancy
inflammatory bowel disease
mechanical perforation
○ trauma
○ colonoscopy
○ foreign bodies
○ iatrogenic
postoperative free intraperitoneal gas
peritoneal dialysis
vaginal "aspiration"
cunnilingus
douching
sudden squatting
postpartum exercises
water-skiing
mechanical ventilation
pneumomediastinum
pneumothorax
24.
Neonatal
Pneumoperitoneum
The causesof neonatal pneumoperitoneum are
different from adult Pneumoperitoneum and include:
perforated hollow viscus
necrotizing enterocolitis (NEC): most common
meconium ileus in cystic fibrosis
Hirsch sprung disease
intestinal atresia or web
peptic ulcer disease
iatrogenic
intubation/mechanical ventilation
rectal thermometer
enema
25.
Upright film
best
• Thepatient should be positioned
sitting upright for 10-20 minutes
prior to acquiring the erect chest X-
ray image.
• This allows any free intra-abdominal
gas to rise up, forming a crescent
beneath the diaphragm. It is said that
as little as 1ml of gas can be detected
in this way.
26.
Radiographic features inPneumoperitoneum
Chest radiograph
An erect chest x-ray is probably
the most sensitive plain
radiograph for the detection of
free intraperitoneal gas.
subdiaphragmatic free gas
leaping dolphin sign
cupola sign (on supine film)
continuous diaphragm sign
Abdominal radiograph
The signs created by the free
intraperitoneal air can be further
divided by anatomical
compartments in relation to the
Pneumoperitoneum:
bowel-related signs
double wall sign (also known as
Rigler sign or bas-relief sign)
telltale triangle sign (also known as
the triangle sign or telltale triangle)
peritoneal ligament-related signs
football sign
falciform ligament sign
lateral umbilical ligament sign (also
known as inverted "V" sign)
urachus sign
right upper quadrant signs
cupola sign
fissure for ligamentum teres sign
hepatic edge sign
lucent liver sign
Morison pouch sign(doge cap sign)
periportal free gas sign
27.
• Air /gasunder the diaphragm in an erect chest xray
The patient has a large volume of free gas under the
diahragm .
Dark crescents have formed separating the thin
diaphragm from the liver on the right and bowel on the
left.
This patient had a perforated duodenal ulcer.
28.
Air /Gas underthe diaphragm close up
If perforation is suspected you must look very closely .
In this patient only a very thin crescent has formed under only
the right hemidiaphragm .
Pneumoperitoneum due to insufflations of gas at laparoscopy
has identical appearances .
29.
Riglers sign alsoknown as double wall sign is the
appearance of lucency (gas) on both sides of the bowel
wall,
Note normally only the inner wall of the bowel is visible
I f the is Pneumoperitoneum both sides of the bowel
wall may be visible
30.
• Supine
• Bowelwall
(extraluminal =
free peritoneal
gas)
of bowel
wall can be seen
(red
arrows)
Index
31.
Rigler’s
Sign
Bowel wall visualisedon both sides due to intra and
extraluminal air Usually large amounts of free air
May be confused with overlapping loops of bowel, confirm with
upright view
Football sign
2 radiographswere required to completely cover the abdomen
in this large patient .
A large volume of free gas has risen to the front of the
peritoneal cavity resulting in a large round black area –’football
sign ‘
The double wall sign (rigler”s ) is also visible .
34.
Liver edge -example (close up)
Gas may be seen outlining soft tissues structures such as
the falciform ligament, or the liver edge
• Supine
• Falciformligament
– connects the
anterior
abdominal wall to
the liver
– extends inferiorly
beyond the liver →
becomes round
ligament
– becomes
in a patient with
free
abdominal gas
Index
•
corner
bord
er outlining the
medialborder of
the liver
4. Positioned inferior
to
the 11thrib
5. Positioned
superior to the
right kidney
Morrison’s pouch =
a potential space
between the right
kidney & the liver Index
Inverted V
sign
• Onthe supine radiograph, an inverted
"V" may be seen over the pelvis in a
patient with pneumoperitoneum.
• While in infants this is produced by
the umbilical arteries, in adults it
appears to be created by the inferior
epigastric vessels
42.
• Supine
• Freeair outlining the
, coursing
inferiorly and
laterally from the
umbilicus
– Infants:
umbilical
arteries
– Adults: inferior
epigastric vessels
Index
• subdiaphragmatic
gas underthe left
hemidiaphragm
– subdiaphragmatic
free gas (under
black arrow)
– normal gas within
the fundus of the
stomach (under
white arrow)
Index
• The lessersac
– positioned
posterior to the
stomach
– usually a potential
space
Note:
White arrow = Cupola
sign
Index
48.
Lesser sac
Sign
Cupola
Sign
Lesser
sac
sign
– (black
arrows)
Thelesser sac is
positioned
posterior to the
stomach and is
usually a
potential space.
There is free
connection
between the
lesser sac and
the greater sac
through the
foramen of
Winslow
Cupol
a
sign
–
(white
arro
ws)
Air superior
to left lobe
of liver
Double Bubble
Sign
49.
• small trianglesof
free gas positioned
between the large
bowel and the flank
Index
50.
• arrowed
NOT clearly
containedwithin
normal hollow
abdominal viscus
– NOT aligned in a
linear fashion nor
outline normal
haustral features
Index
51.
• Air contrasted
urachus
•Vertical line
between bladder
and umbilicus
• Outline of
medial
umbilical
ligament
Index
• Extraluminal airin
the fissure for the
Ligamentum Teres
• Linear density
running along the
inferior edge of
the falciform
ligament
Emerg Med J
2011;28:728
Picture: DOI:
10.1056/NEJMicm0904627 Index
54.
Pneumoretroperitoneum
Pneumoretroperitoneum isby
definition presence of gas within
the retroperitoneal space.
Pathology
Pneumoretroperitoneum is always
abnormal and has a relatively small
differential:
perforated retroperitoneal hollow
viscus
rarely an intraperitoneal hollow viscus
can perforate into the intramesenteric
space and then track air to the
retroperitoneal spaces
residual air from retroperitoneal
surgery
urological/adrenal
spinal (anterolateral approach)
If localised, and especially in the
presence of an air-fluid level, a
retroperitoneal abscess should be
suspected.
Radiographic features
Pneumoretroperitoneum is best
appreciated by CT, however, can
also be detected by plain abdominal
radiograph and even by
transabdominal ultrasound.
Generally, the air is most commonly
seen surrounding the kidneys in the
right and left upper quadrants of
the abdomen 6
. There may also be a
loss of the normal psoas muscle
shadow
55.
• Air seen
surroundingthe
lateral border of the
kidney
(retroperitoneal
organs)
• If the gas is seen
to move in an
erect and
decubitus view, it's
in the
retroperitoneum Index
56.
INTRAMURAL BOWEL GAS/PNEUMATOSIS
INTESTINALIS
Intramural bowel gas, also known as pneumatosis intestinalis, refers to
the clinical or radiological finding of gas within the wall of the bowel.
Terminology : pneumatosis coli and pneumatosis cystoides intestinalis.
Pneumatosis coli is used when only the colic wall is involved and is generally
an incidental finding in asymptomatic patients.
Pneumatosis cystoides intestinalis is descriptive for multiple gaseous cysts
along the bowel wall.
Pathology
Intramural gas can be seen in intestinal ischaemia and eventually bowel
infarction. This is the most concerning aetiology for intramural gas.
Gas in the bowel wall in the neonatal period, whatever its shape, is
diagnostic of necrotising enterocolitis.
Asymptomatic pneumatosis intestinalis may result from a variety of
interrelated contributing factors including:
mucosal integrity
intraluminal pressure
bacterial flora
intraluminal gas
57.
Due todisruption in mucosal integrity with increased
mucosal permeability, gas-forming bacteria can enter
the submucosa and can produce predominantly
hydrogen gas. Another theory is mechanical pressure
from pulmonary diseases like COPD leads to
pneumatosis intestinalis.
Benign pneumatosis can be caused by a variety of
reasons such as pulmonary disease, systemic disease
(scleroderma, lupus ,AIDS), intestinal inflammation,
iatrogenic/procedures, medications (steroids,
chemotherapeutic drugs, lactulose, sorbitol and
voglibose), and organ transplantation 4
.
Life-threatening pneumatosis can be caused by
intestinal ischaemia, obstruction, enteritis/colitis, toxic
caustic ingestion, toxic megacolon, organ
transplantation, and collagen vascular disease
Pneumobilia
Pneumobilia, alsoknown as
aerobilia, is the accumulation
of gas in the biliary tree.
It is important to distinguish
pneumobilia from portal
venous gas, the other type of
branching hepatic gas.
Aetiology
recent biliary instrumentation
ERCP
common bile duct stent
placement (normal finding,
indicating patency of the stent)
percutaneous transhepatic or
intraoperative cholangiography
(small amount of gas only)
incompetent sphincter of
Oddi
sphincterotomy
following passage of a gallstone
scarring e.g. chronic
pancreatitis
drugs e.g. atropine
congenital
biliary-enteric surgical
anastomosis
cholecystoenterostomy
choledochoduodenostomy
Whipple procedure
60.
spontaneous biliary-entericfistula
gallstone ileus
peptic ulcer disease
traumatic
neoplasm, eg. Cholangiocarcinoma, ampullary cancer
infection (rare)
cholangitis
emphysematous cholecystitis
liver abscess (if contains gas and communicates with the biliary tree)
ruptured hydatid cyst
biliary-bronchopleural fistula (rare)
Radiographic features
Pneumobilia is typically seen as linear branching gas within
the liver most prominent in central large calibre ducts as the
flow of bile pushes gas toward the hilum. This is in contrast to
portal venous gas where peripheral small calibre branching
gas is usually seen due to the hepatopetal flow of blood away
from the hilum.
61.
Air in thebiliary
tree
• One or two tube-like branching
lucencies in the RUQ, conform to
location of major bile ducts
62.
Biliary vs Portal
VenousAir
• Portal venous air
usually
associated with
bowel necrosis
• Air is peripheral
rather than
central
• Numero
us
branchin
g
structure
63.
Free airgas mimics
1. The normal stomach burble
2. Chilaiditis sign
3. False football sign
64.
Normal stomach bubble- erect chest X-ray
Round/ovoid - 'bubble' shape
Thick upper wall
Fluid level or food contents
65.
Chilaiditis
sign
•
•
•
May mimic air
underthe
diaphragm
Look for haustral
folds
Get left lateral
decubitus to
confirm
In patients who have
cirrhosis or flattened
diaphragms due to lung
hyperinflation, a void is
created within the upper
abdomen above the liver. This
space may be filled by bowel.
If this bowel is air filled then
it may mimic free gas.
66.
Chilaiditi's phenomenon -example
Gas forms a near crescent shape under the right
hemidiaphragm
There is however a thick hemidiaphragm (partly consisting of
bowel wall)
Gas can be seen to lie within bowel
Importantly, this patient with hyperexpanded lungs, due to
emphysema, did not have acute abdominal pain
67.
False Rigler's/double wallsign
Gas seen on both sides of the bowel wall is contained within adjacent bowel
There are no black triangles or sharp angles on the outside of the bowel wall
68.
False football sign- example
1 - Perirenal fat (retroperitoneal)
2 - Peritoneal fat (next to the liver)
3 - Abdominal wall fat (separating muscles of the
abdominal wall)
SMALL BOWEL
OBSTRUCTION
Smallbowel obstruction (SBO) accounts for 80% of all
mechanical intestinal obstruction, the remaining 20% results
from a large bowel obstruction.
Clinical presentation
Classical presentation is cramping abdominal pain and
abdominal distension with nausea and vomiting.
Radiographic findings can be evident 6-12 hours before the
onset of clinical symptoms .
Pathology
Causes can be divided into congenital and acquired. Acquired
causes may be extrinsic causing compression, intrinsic, or
luminal.
In developed countries, adhesions are by far the most common
cause, accounting for ~75% of obstructions while in developing
countries incarcerated hernias are much more common
accounting for 80% of obstructions .
71.
CONGENITAL CAUSES
1.Jejunal atresia
2. ileal atresia or stenosis
3. enteric duplication
4. midgut volvulus
5. mesenteric cyst
6. Meckel diverticulum
Extrinsic causes
fibrous adhesions
main cause in developed countries (75% of cases)
almost all are related to post-operative adhesions with a small
percentage secondary to peritonitis
diagnosis of exclusion as adhesive bands are not seen on CT
abrupt change in calibre without mass lesion, inflammation or
bowel wall thickening at transition point
72.
abdominal hernia
10% of cases in developed countries
external hernia related to abdominal or pelvic wall defect (congenital
weakness or previous surgery)
internal hernia with protrusion of viscera through peritoneum or
mesentery into another abdominal compartment
endometriosis
rare cause of SBO
endometrial implants are typically on anti-mesenteric edge of the
bowel
solid enhancing nodule contiguous with or penetrating the thickened
bowel wall
may infiltrate the submucosa with a hypoattenuating layer between
the muscularis and mucosa
masses
extrinsic neoplasm
intra-abdominal abscess
aneurysm
haematoma
73.
Intrinsic bowelwall causes
inflammation, e.g. Crohn, tuberculosis, eosinophilic
gastroenteritis
small bowel obstruction in Crohn disease may relate to:
○ acute flare with luminal narrowing secondary to transmural inflammation
○ cicatricial stenosis in long-standing disease
○ adhesions or incisional hernias from previous surgery
tumour (rare)
primary small bowel neoplasms are rare and usually advanced at the
time of SBO.
○ GIST adenocarcinoma, lymphoma.
○ asymmetric and irregular mural thickening at the transition point
small bowel involvement of metastatic disease is more common
○ peritoneal carcinomatosis with an extrinsic serosal disease in association with
the transition point
caecal malignancy involving ileocaecal valve
radiation enteritis
produces adhesive and fibrotic changes in the mesentery with luminal
narrowing and dysmotility
may cause an obstruction in the late phase (>1 year after therapy)
74.
intestinal ischaemia
occlusion or stenosis of the mesenteric arterial or vascular supply
produces small bowel wall thickening and obstruction
Pneumatosis and portal venous gas if advanced
intramural haematoma
trauma, iatrogenic, anticoagulant therapy, Henoch-Schonlein
purpura
produces luminal narrowing
better seen on non-enhanced CT with homogenous, regular and
spontaneously hyper-attenuating wall
intussusception
rare in adults (<5% of SBO)
lead point may relate to neoplasm, adhesion or foreign body
bowel-within-bowel with or without mesenteric fat and mesenteric
vessels
leading mass should be carefully interpreted and differentiated
from the soft-tissue pseudotumour that represents the
intussusception itself
75.
Intraluminal causes
swallowed, e.g. foreign body, bezoar
gallstone ileus
rare complication of recurrent cholecystitis
biliary-intestinal fistula with impaction of a
gallstone in the small bowel
meconium ileus (or meconium ileus
equivalent, distal intestinal obstruction
syndrome)
migration of gastric balloon
76.
Radiographic features
Abdominal radiograph
Abdominal radiographs are only 50-60% sensitive for small bowel
obstruction
In most cases, the abdominal radiograph will have the following
features:
dilated loops of small bowel proximal to the obstruction
predominantly central dilated loops
three instances of dilatation > 2.5 - 3 cm
valvulae conniventes are visible
gas-fluid levels if the study is erect, especially suspicious if
>2.5 cm in width
in the same loop of bowel but at different heights (> 2 cm difference in height)
However, obstruction (which may be high-grade mechanical
obstruction) may also present with the following features:
gasless abdomen: gas within the small bowel is a function of vomiting,
NG tube placement and level of obstruction
string-of-beads sign: small pockets of gas within a fluid-filled small
bowel
String of pearls
sign
Considereddiagnostic of obstruction (as opposed to
ileus) and is caused by small bubbles of air trapped in
the valvulae of the small bowel.
Small bowel obstruction- features
Centrally located multiple dilated loops of gas filled bowel .
Valvulae conniventes are visible - confirming this is small bowel
Evidence of previous surgery - note the anastomosis site - this
suggests adhesions is the likely cause of obstruction
(confirmed at surgery
86.
Closed loop
obstruction
• Twopoints of same loop of bowel
obstructed at a single location
• Forms a C or a U shape
– Term applies to small bowel, usually
caused by adhesions
– Large bowel, called a volvulus
87.
Localised
ileus
•
•
•
•
•
Key
features
One or twopersistently
dilated loops of small or
large bowel (multiple
views)
Often air-fluid levels in
sentinel loops
Local irritation, ileus in
same anatomical region
as pathology
Gas in rectum or
88.
Causes of Localised
Ileus
bylocation
SITE OF DILATED LOOPS CAUSE
Right upper
quadrant Left
upper quadrant
Right lower
quadrant Left
lower quadrant
Mid-abdomen
Cholecystit
is
Pancreatiti
s
Appendicit
is
Diverticulit
is
89.
Colon cut off
sign
Abruptcutoff of colonic gas column at the splenic flexure (arrow). The
colon is usually decompressed beyond this point.
Explanation:
Inflammatory exudate in acute
pancreatitis extends into the
phrenicocolic ligament via
lateral attachment of the
transverse mesocolon
Infiltration of the phrenicocolic
ligament results in functional
spasm and/or mechanical
narrowing of the splenic flexure
at the level where the colon
returns to the
retroperitoneum.
90.
Sentinel loop
A localizedloop of small bowel is dilated in this patient with acute pancreatitis
This appearance is not diagnostic of intra-abdominal inflammation, but rather
an occasional associated feature
91.
Generalised
ileus
Key features
• Entirebowel aperistaltic/hypoperistaltic
• Dilated small bowel and large bowel to
rectum (with LBO no gas in
rectum/sigmoid)
• Long air-fluid levels
CAUSE REMARK
*Postoperative Usually abdominal
surgery
Electrolyte imbalance Diabetic ketoacidosis
* almost always
92.
Post operative ileus
Appearancesare similar to those of mechanical
obstruction
There are multiple loops of gas filled bowel projected
centrally over the abdomen
This patient had prolonged non-colicky abdominal
pain following a Caesarian section - recovery was
spontaneous
Large bowelobstruction (LBO) is often impressive on
imaging, on account of the ability of the large bowel to
massively distend.
This condition requires prompt diagnosis and treatment.
Large bowel obstructions are far less common than small
bowel obstructions, accounting for only 20% of all bowel
obstructions .
The classic presentation is with abdominal pain, distension,
and failure of passage of flatus and stool.
As dilatation of the colon increases, the risk of perforation
also increases.
Perforation may occur at the site of obstruction, or more
proximally secondary to ischaemic change, which may be
implied by the presence of intramural gas or decreased mural
enhancement.
Signs of peritonis, sepsis, and shock may develop when
perforation occurs.
96.
Pathology
Theunderlying aetiology of large bowel
obstructions is age-dependant, but in
adulthood, the most common cause is colonic
cancer (50-60%), typically in the sigmoid .
The second most common cause in adults is
acute diverticulitis (involving the sigmoid
colon).
Together, obstructing tumors and acute
diverticulitis account for 90% of all causes of
large bowel obstruction.
While adhesions are the leading cause of small
bowel obstruction, for practical purposes, they
do not tend to cause large bowel obstruction.
97.
MALIGNANCY
colorectal
carcinoma (most
common,50-60%)
pelvic tumours; direct
spread or metastatic
disease
colonic diverticulitis
volvulus
caecal volvulus (1-3%)
caecal bascule
sigmoid volvulus (3-
8%)
ischaemic stricture
faecal
impaction/faecaloma
(most common cause
in debilitated elderly)
hernias (uncommon)
intussusception
98.
Radiographic features
Large bowel obstructions are characterized by
colonic distension proximal to the obstruction,
with collapse distally.
In some cases, the point of obstruction and site of
obstruction are not the same, with the point of
obstruction located distal to the apparent cut-off
point, e.g. an obstructing sigmoid tumour may
present with an apparent cut-off at the splenic
flexure.
In general the colon is considered dilated if it is
over 6 cm in diameter, with the caecum having an
upper limit of 9 cm .
A caecal diameter of 12 to 15 cm increases the
risk for caecal rupture .
99.
Plain radiograph
colonic distension: gaseous secondary to gas-producing
organisms in faeces
collapsed distal colon: very few or no air-fluid levels are found
in the large bowel because water is reabsorbed .
small bowel dilatation, which depends on
duration of obstruction
incompetence of the ileocaecal valve
rectum has little or no air
In advanced cases one may see the stigmata of an ischaemic
colon, namely:
intramural gas (pneumatosis coli)
portal venous gas
free intra-abdominal gas (pneumoperitoneum)
100.
Large bowel obstruction
Herethe colon is dilated down to the level of the distal descending colon.
There is the impression of soft tissue density at the level of obstruction (X).
No gas is seen within the sigmoid colon.
Obstruction is not absolute in this patient as a small volume of gas has
reached the rectum .
An obstructing colon carcinoma was confirmed on CT and at surgery.
101.
Mechanical
LBO
• Colon dilatesfrom
point of obstruction
backwards
• Little/no air fluid
levels (colon
reabsorbs water)
• Little or no air
in
rectum/sigmo
id
102.
Large bowel
obstruction
Bowel loopstend not
to overlap therefore
possible to identify
site of obstruction
Little or no gas in
small bowel if
ileocaecal valve
remains competent*
* If incompetent, large bowel
decompresses into small bowel,
may look like SBO
103.
Large vs small
bowel
•Large bowel
– Peripheral (except RUQ occupied by liver)
– Haustral markings don’t extend from wall
to wall
• Small bowel
– Central
– Valvulae conniventes extend across lumen
and are spaced closer together
104.
Note on
volvulus
• Sigmoidcolon has its own mesentry
therefore prone to twisting
• Caecum usually retroperitoneal and not
prone to twisting; 20% people have
defect in peritoneum that covers the
caecum resulting in a mobile caecum
105.
Volvul
us
A volvulus alwaysextends away from the area of
twist. Sigmoid volvulus can only move upwards and
usually goes to the right upper quadrant. Caecal
volvulus
can go almost anywhere.
106.
Sigmoid volvulus -'coffee bean' sign
The sigmoid colon is very dilated because it is twisted at the root of its
mesentery in the left iliac fossa (LIF). The proximal large bowel is also
dilated (asterisks).
The twisted loop of sigmoid colon is said to resemble a coffee bean. As
in this case the loop of dilated sigmoid colon - or 'coffee bean' - usually
points upwards towards the diaphragm.
This patient is at high risk of perforation and/or bowel ischaemia.
Caecal volvulus
The massivelydilated caecum no longer lies in the right iliac
fossa (RIF). Rather this is occupied by small bowel (red outline).
The small bowel is identified by the valvulae conniventes -
mucosal folds that cross the full width of the bowel
(arrowheads). Caecal volvulus was confirmed at laparotomy
109.
Bowel wallinflammation
Occasionally, abdominal X-rays show
signs of inflammation in patients with
inflammatory bowel disease.
Abnormalities may relate to either
acute or chronic stages of disease.
110.
Mucosal thickening -'thumbprinting'
This patient presented with an exacerbation of symptoms of
ulcerative colitis.
The distance between loops of bowel is increased (arrows) due to
thickening of the bowel wall. The haustral folds are very thick
(arrowheads), leading to a sign known as 'thumbprinting
111.
Thumbprint
ing
The distance between
loopsof bowel is
increased due to
thickening of the bowel
wall.
The haustral folds are
very thick, leading to a
sign known as
'thumbprinting.'
112.
Lead pipe colon
Thispatient with ulcerative colitis has a featureless segment of
transverse colon with loss of the normal haustral markings.
This 'lead pipe' appearance is associated with longstanding ulcerative
colitis.
The distal bowel is always involved in this disease but, as there is no air in
the descending colon, this segment of colon is not evidently abnormal.
Toxic megacolon
The colonis very dilated in this patient with acute abdominal
pain, sepsis, and a known history of ulcerative colitis. The
clinical features and X-ray appearances are consistent with toxic
megacolon.
There is evidence of bowel wall oedema with 'thumbprinting',
and pseudopolyps or 'mucosal islands' (red-patches).
115.
3, 6, 9RULE
Maximum Normal Diameter of
bowel
Small bowel 3cm
Large bowel 6cm
Caecum
Soft tissue masses
•Organomegaly
– Know normal landmarks
2 ways to identify soft tissue
masses/organs:
– Direct visualisation of edges of
structure
– Indirect by displacement of bowel
CT, US and MRI have essentially replaced
conventional radiography in the assessment of
organomegaly and soft tissue masses
118.
Lung bases
This patienthad pseudo-obstruction (note the
dilated bowel) secondary to a left basal pneumonia
The image shows consolidation and a loculated
pleural effusion at the left lung base
119.
Hepatomegaly
There is diffusesoft tissue density shadowing in the
right upper quadrant due to hepatomegaly (liver
enlargement)
The enlarged liver has displaced the normal bowel
downwards and to the left (arrows)
The spleen is also mildly enlarged
120.
Massive splenomegaly
This patientwith a myeloproliferative disorder has both
hepatomegaly and massive splenomegaly
There is generalised increase in soft tissue density but the bowel
appears pushed away by the edge of the spleen
121.
Enlarged kidneys
Both kidneysare very enlarged
The bowel is not displaced because the kidneys are
retroperitoneal structures
This patient had a family history of polycystic kidneys
This diagnosis was confirmed with ultrasound
122.
Ascites
There is generalizedhazy density of the entire abdomen
A loop of gas filled bowel lies centrally in the abdomen
123.
Pelvic mass -large
A very large soft tissue density mass extends upwards from the pelvis
Bowel is displaces superiorly in the abdomen
124.
Pelvic mass -small
A right pelvic wall mass is easily missed
If you see a mass on an abdominal X-ray - re-examine the patient before
planning further imaging
125.
Pelvic fracture andosteoarthritis
This elderly patient presented with abdominal pain with no clear
history of trauma
Tenderness in the suprapubic regions was thought to be due to
intra-abdominal pathology
The pubic ramus fractures was the cause of symptoms
Note the osteoarthritic appearances of the hips and lumbar spine
126.
Bone metastases
There arenumerous sclerotic densities
(white) of the vertebrae, sacrum, pelvis and
proximal femora
This patient had a known history of breast
cancer
Abdominal pain was actually due to high
127.
Paget's disease
This patienthas Paget's disease which affects his lumbar spine
and right hemipelvis
This was an incidental finding when looking for a cause of
abdominal pain
The typical features of Paget's are bone expansion and
coarsening of the trabecular pattern involving the whole of the
bone(s) affected
128.
Bone andsoft tissue disease are
encountered incidentally on
abdominal X-rays
Awareness of the abnormalities you
may encounter helps avoid confusion
Ultrasound or dedicated X-rays are
required for initial investigation of
suspected abdominal soft tissues or
bone disease
Rim-
like
• Calcification thathas occurred in the
wall of a hollow viscus
– Cysts
• renal, splenic, hepatic
– Aneurysms
• aortic, splenic, renal
artery
– Saccular organs
• Gallbladder
• Urinary bladder
Calcified hydatid
cysts
131.
Renal calcification
Abnormal renal calcification may affect either the renal parenchyma
(nephrocalcinosis) or more commonly the collecting system (renal
calculi).
Pelvicalyceal calcification
Renal stones/calculi are concretions of inorganic material within the
renal collecting system. 90% of renal calculi contain enough calcium to
be visible on abdominal X-rays.
Urate and matrix stones are not visible.
Renal stones are often small, but if large can fill the renal pelvis or a
calyx, taking on its shape which is likened to a staghorn.
Other investigations
Renal calculi may be visible on the 'control' study of an intravenous
urogram (IVU)
Renal calculi may also be visible with ultrasound, or CT of the Kidneys,
Ureters and Bladder (CT-KUB
Nephrocalcinosis
Uncommonly the renalparenchyma can become calcified. This is
known as nephrocalcinosis, a condition found in disease entities
such as hyperparathyroidism or medullary sponge kidney
The renal parenchyma contains clusters of small calcific densities
134.
Nephrocalcinosis
Uncommonly the renal
parenchymacan
become calcified.
This is known as
nephrocalcinosis, a
condition found in disease
entities such as medullary
sponge kidney or
hyperparathyroidism.
Renal calculi
Parenchymal
calcification
Flocculen
t
135.
Putty
Kidney
• "Putty kidney"
–sacs of
casseous,
necrotic
material (TB)
• Autonephrect
omy
– small,
shrunken
kidney with Flocculen
t
Bladder stones generallyform in the bladder itself. They arise as a result of
urinary stasis such as in bladder outflow obstruction (enlarged prostate) or
in patients with a neurogenic bladder (loss of bladder function due to spinal
cord injury/disease). Those with bladder wall abnormalities (ureterocele,
diverticulum) or those with recurrent urinary infections are also at higher
risk of forming bladder stones.
Multiple well defined calcific densities are seen within the bladder
138.
Vascular calcification.
Occasionally vascularcalcification seen on an abdominal X-ray reveals an
unexpected aneurysm.
Remember that abdominal pain is not only caused by gastrointestinal
disease.
There is striking calcification of the aorta and iliac vessels
This is a sign of generalised atherosclerosis elsewhere in the body
139.
Abdominal aortic aneurysm- AAA
There is calcification of the dilated aortic wall
Frequently only one side of the aneurysm is
visible - as in this image - the other being
projected over the spine
140.
Pancreatic calcification isa sign of chronic pancreatitis
Chronic pancreatitis
This X-ray shows soft tissue calcification which follows the
anatomical position of the pancreas
Also note calcification of the abdominal aorta which is of
normal calibre
141.
Adrenal (suprarenal) calcificationis an uncommon finding
and is usually incidental. Most often it is considered a result
of previous haemorrhage or tuberculosis.
Adrenal calcification
The adrenal (suprarenal) glands form a triangle shape lying
directly above the kidneys
142.
The gallbladder andhence gallstones have a variable position
Most gallstones are asymptomatic
Gallstones and mesenteric lymph node
Gallstones have a variable position depending on the position of the
gallbladder and may be mistaken for renal stones
Unlike renal stones they are often rounded and cluster together
This X-ray also shows an incidental calcified mesenteric node which may also
mimic renal stones
143.
Appendicolith is anoccasional but important X-ray
feature of appendicitis
Appendicoliths are highly predictive of appendicitis in
patients presenting with right iliac fossa pain
144.
Linear/
Track
• Calcification inwalls of tubular
structures
Aortoiliac calcification
– Arteries
– Fallopian tubes
– Vas deferens
– Ureter
Naso-jejunal tube
Placed forthe purpose of enteral feeding
The tube passes through the stomach and forms a C-
shape as it navigates the 4 parts of the duodenum (D1-4)
The tube tip lies beyond the duodenojejunal flexure which
lies on the left
150.
Pig-tail (JJ) stent
Aureteric stent has been placed to relieve
ureteric obstruction
The catheter has loops (pig-tails) at both ends
which hold it in place
151.
Colonic stent
Large bowelobstruction can be treated with
placement of a metallic colonic stent
This is often used as a temporary measure
allowing a patient to recover from the effects of
obstruction prior to definitive colonic resection
152.
Inferior vena cava(IVC) filter
An IVC filter may be used to reduce the risk of large pulmonary emboli
Most commonly used in patients who have had pulmonary embolism but for whom
anticoagulation is contraindicated
IVC filters are self-expanding wire structures shaped like an umbrella
Small clots may pass between the wires of the filter but large clots are prevented
from reaching the pulmonary arteries
153.
Foreign body -ingested
This psychiatric patient has ingested
numerous radio-opaque objects
The navel jewellery is external!
154.
Conclusi
on
• Approach toAXR should include gas
pattern, extraluminal air, soft tissue
and calcifications
• Named radiological signs are a useful
way of remembering, identifying and
reporting on films









































































































































































































![carotid stenosis [Autosaved].pptx for master students](https://cdn.slidesharecdn.com/ss_thumbnails/carotidstenosisautosaved-241229032708-f20dd02c-thumbnail.jpg?width=640&height=640&fit=bounds)



















