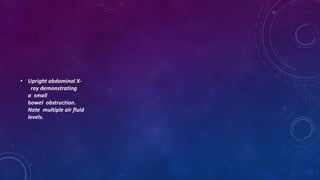
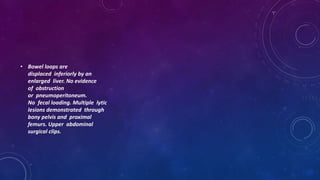
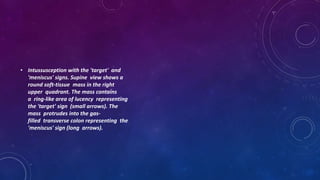
This document provides an overview of interpreting abnormal x-rays of the abdomen using the ABCDE approach. It describes how to identify air in abnormal locations, abnormalities of the bowel loops including dilation and inflammation. It also discusses identifying dense structures like bones and calcifications. Specific conditions covered include pneumoperitoneum, pneumoretroperitoneum, pneumobilia, bowel obstructions, volvulus, and calcifications. Radiographic signs are provided for many of these conditions.










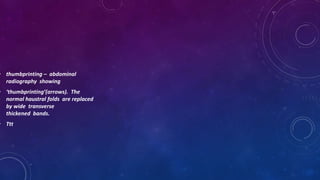
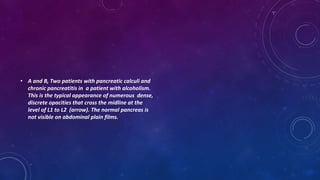
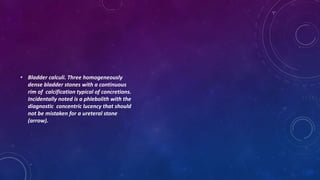






























![ankle MRI.pptx [Repaired].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/anklemri-230430061225-0fe22f3a-thumbnail.jpg?width=640&height=640&fit=bounds)


























