HOW TO READAN X-RAY
Properties of an x-ray image
• It is an grey scale
• It is summations of shadows
• It is two dimensional representation of a three
dimensional concept
• It is a static representation of a dynamic disease
process interpret with history, laboratory findings,
serial image findings
4.
HOW TO READAN XRAY IMAGE
• Elements of visual search
• Elements of detection
• Elements of interpretation
– A thorough knowledge of anatomy pathology,
Pathoanatomy pathophisiology of the disease
process with statistical guidance is essential to
come to a reasonable diagnosis
5.
BASIC DENSITIES
• Air= black
• Fat = dark grey
• Soft tissue/fluid = light grey
• Bone/calcification = white
• Metal = intense white
6.
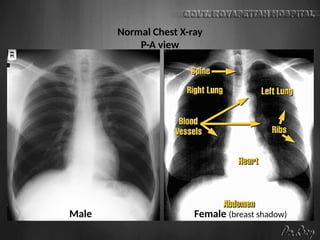
CHEST X-RAY PAVIEW
• Commonest of all x-ray investigations
performed in the department
• It is considered a routine but in fact it is the
most essential first x-ray examination
• Most of the diseases systemic pulmonary or
cardiac can be diagnosed by a glimpse
through this window
7.
INDICATIONS
• In AllDiseases Of The Chest ( Chestwall Lung Heart & Mediastinum)
• To The Check The Correct Placement Of Tubes, Electrodes And Other
Monitoring Devices
• Mass Minature Screening Of Communicable Diseases Like Tb
• Pyrexia Of Unknown Origin
• Preoperative Assesment Before General Anesthesia
• For Immigration And Health Care Screening
• In Other Systemic Or General Diseases With Suspected Lung
Involvement
8.
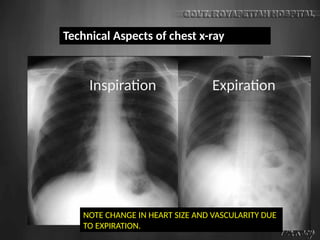
NOTE CHANGE INHEART SIZE AND VASCULARITY DUE
TO EXPIRATION.
Technical Aspects of chest x-ray
Inspiration Expiration
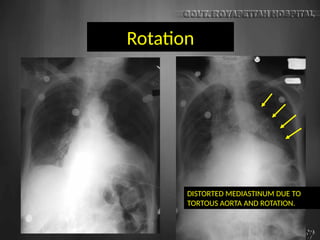
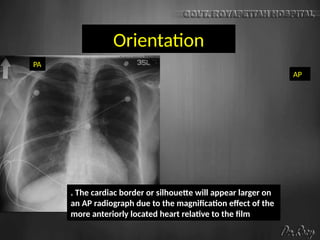
Orientation
PA
AP
. The cardiacborder or silhouette will appear larger on
an AP radiograph due to the magnification effect of the
more anteriorly located heart relative to the film
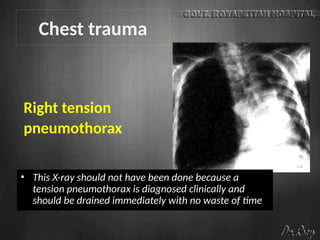
Right tension
pneumothorax
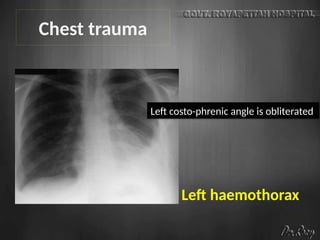
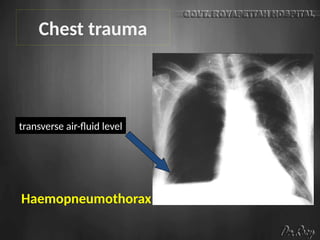
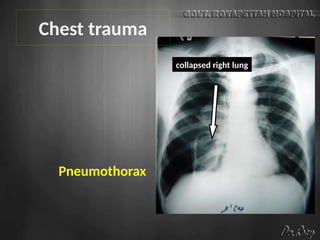
Chest trauma
•This X-ray should not have been done because a
tension pneumothorax is diagnosed clinically and
should be drained immediately with no waste of time
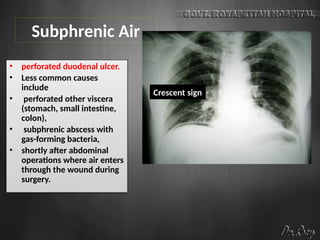
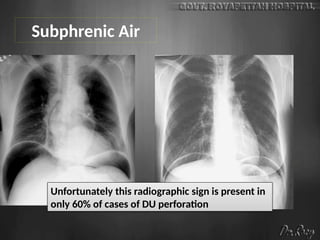
Subphrenic Air
• perforatedduodenal ulcer.
• Less common causes
include
• perforated other viscera
(stomach, small intestine,
colon),
• subphrenic abscess with
gas-forming bacteria,
• shortly after abdominal
operations where air enters
through the wound during
surgery.
Crescent sign
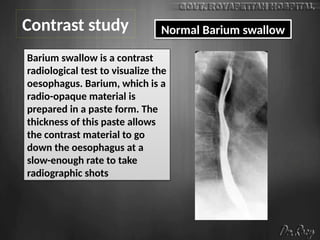
Contrast study NormalBarium swallow
Barium swallow is a contrast
radiological test to visualize the
oesophagus. Barium, which is a
radio-opaque material is
prepared in a paste form. The
thickness of this paste allows
the contrast material to go
down the oesophagus at a
slow-enough rate to take
radiographic shots
22.
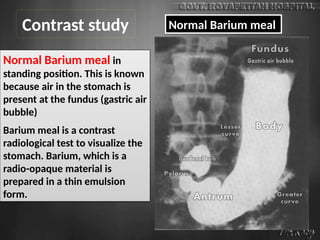
Normal Barium mealin
standing position. This is known
because air in the stomach is
present at the fundus (gastric air
bubble)
Barium meal is a contrast
radiological test to visualize the
stomach. Barium, which is a
radio-opaque material is
prepared in a thin emulsion
form.
Contrast study Normal Barium meal
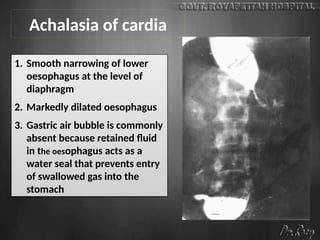
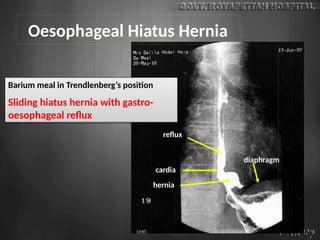
1. Smooth narrowingof lower
oesophagus at the level of
diaphragm
2. Markedly dilated oesophagus
3. Gastric air bubble is commonly
absent because retained fluid
in the oesophagus acts as a
water seal that prevents entry
of swallowed gas into the
stomach
Achalasia of cardia
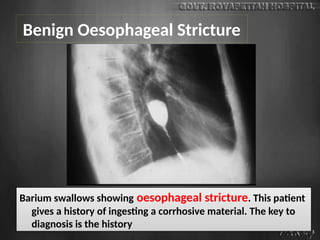
Benign Oesophageal Stricture
Bariumswallows showing oesophageal stricture. This patient
gives a history of ingesting a corrhosive material. The key to
diagnosis is the history
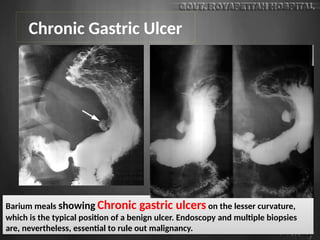
Chronic Gastric Ulcer
Bariummeals showing Chronic gastric ulcers on the lesser curvature,
which is the typical position of a benign ulcer. Endoscopy and multiple biopsies
are, nevertheless, essential to rule out malignancy.
30.
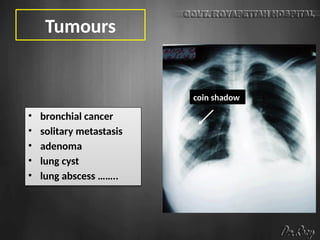
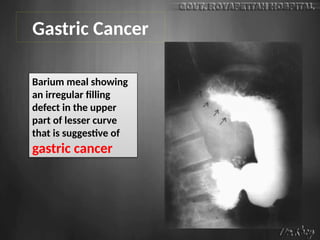
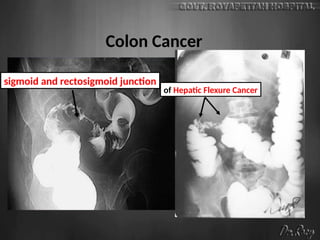
Gastric Cancer
Barium mealshowing
an irregular filling
defect in the upper
part of lesser curve
that is suggestive of
gastric cancer
31.
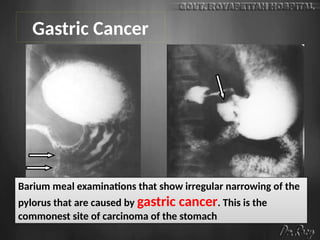
Barium meal examinationsthat show irregular narrowing of the
pylorus that are caused by gastric cancer. This is the
commonest site of carcinoma of the stomach
Gastric Cancer
32.
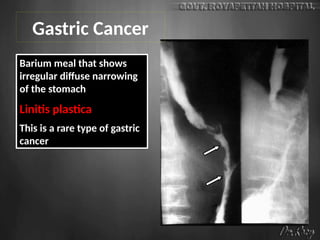
Barium meal thatshows
irregular diffuse narrowing
of the stomach
Linitis plastica
This is a rare type of gastric
cancer
Gastric Cancer
33.
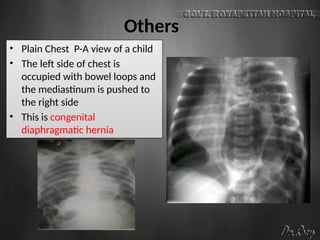
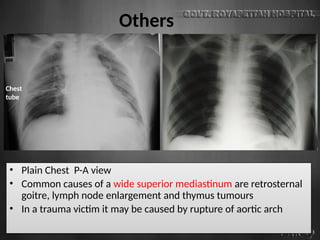
Others
• Plain ChestP-A view of a child
• The left side of chest is
occupied with bowel loops and
the mediastinum is pushed to
the right side
• This is congenital
diaphragmatic hernia
34.
Others
• Plain ChestP-A view
• Common causes of a wide superior mediastinum are retrosternal
goitre, lymph node enlargement and thymus tumours
• In a trauma victim it may be caused by rupture of aortic arch
Chest
tube
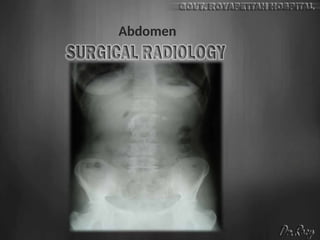
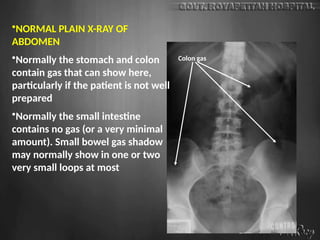
•NORMAL PLAIN X-RAYOF
ABDOMEN
•Normally the stomach and colon
contain gas that can show here,
particularly if the patient is not well
prepared
•Normally the small intestine
contains no gas (or a very minimal
amount). Small bowel gas shadow
may normally show in one or two
very small loops at most
Colon gas
40.
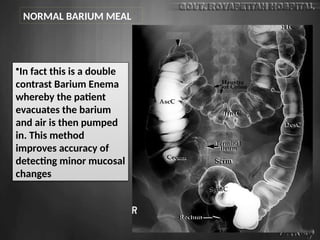
•In fact thisis a double
contrast Barium Enema
whereby the patient
evacuates the barium
and air is then pumped
in. This method
improves accuracy of
detecting minor mucosal
changes
NORMAL BARIUM MEAL
41.
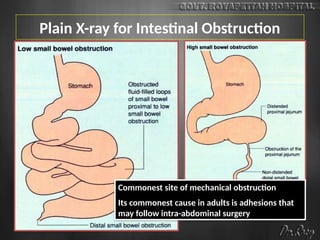
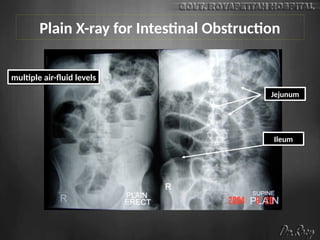
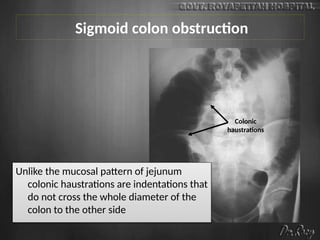
Plain X-ray forIntestinal Obstruction
Commonest site of mechanical obstruction
Its commonest cause in adults is adhesions that
may follow intra-abdominal surgery
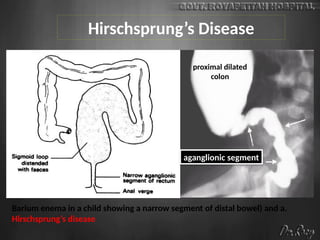
Hirschsprung’s Disease
colon
Barium enemain a child showing a narrow segment of distal bowel) and a.
Hirschsprung’s disease
aganglionic segment
proximal dilated
colon
48.
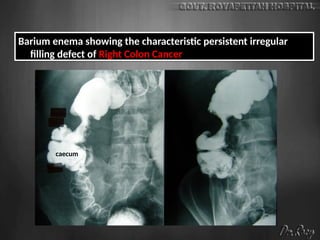
Barium enema showingthe characteristic persistent irregular
filling defect of Right Colon Cancer
caecum
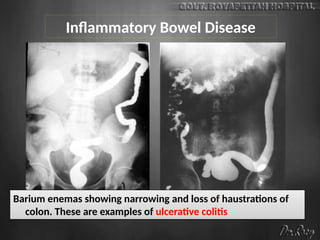
Inflammatory Bowel Disease
Bariumenemas showing narrowing and loss of haustrations of
colon. These are examples of ulcerative colitis
51.
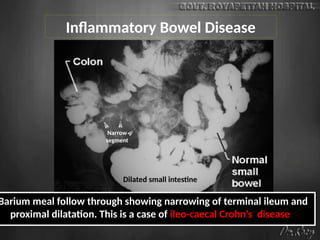
Inflammatory Bowel Disease
Dilatedsmall intestine
Narrow
segment
Barium meal follow through showing narrowing of terminal ileum and
proximal dilatation. This is a case of ileo-caecal Crohn’s disease
52.
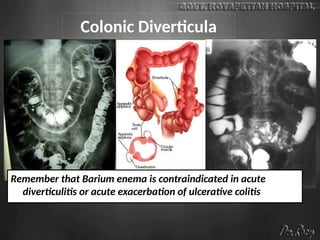
Colonic Diverticula
Remember thatBarium enema is contraindicated in acute
diverticulitis or acute exacerbation of ulcerative colitis
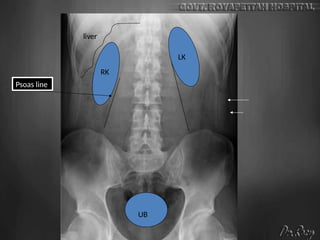
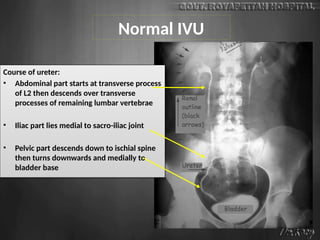
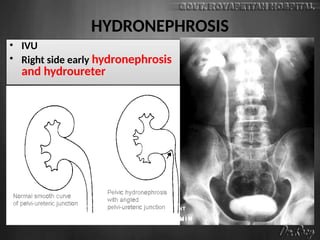
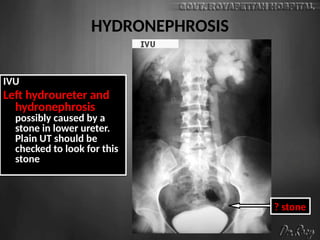
Normal IVU
Course ofureter:
• Abdominal part starts at transverse process
of L2 then descends over transverse
processes of remaining lumbar vertebrae
• Iliac part lies medial to sacro-iliac joint
• Pelvic part descends down to ischial spine
then turns downwards and medially to
bladder base
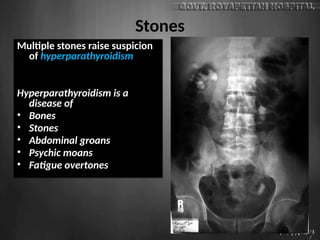
Stones
Multiple stones raisesuspicion
of hyperparathyroidism
Hyperparathyroidism is a
disease of
• Bones
• Stones
• Abdominal groans
• Psychic moans
• Fatigue overtones
60.
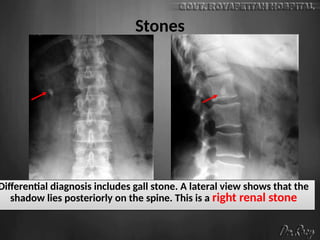
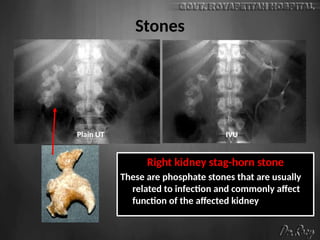
Stones
Right kidney stag-hornstone
These are phosphate stones that are usually
related to infection and commonly affect
function of the affected kidney
Plain UT IVU
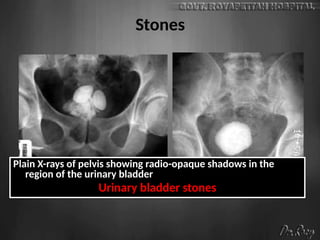
Stones
Plain X-rays ofpelvis showing radio-opaque shadows in the
region of the urinary bladder
Urinary bladder stones
63.
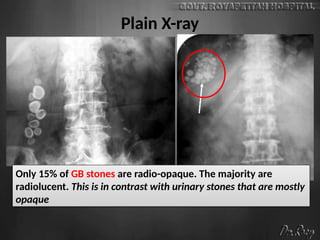
Plain X-ray
Only 15%of GB stones are radio-opaque. The majority are
radiolucent. This is in contrast with urinary stones that are mostly
opaque
64.
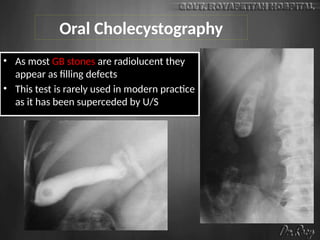
Oral Cholecystography
• Asmost GB stones are radiolucent they
appear as filling defects
• This test is rarely used in modern practice
as it has been superceded by U/S
65.
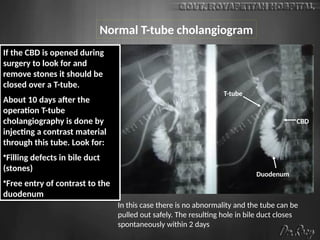
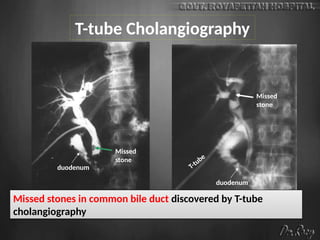
If the CBDis opened during
surgery to look for and
remove stones it should be
closed over a T-tube.
About 10 days after the
operation T-tube
cholangiography is done by
injecting a contrast material
through this tube. Look for:
•Filling defects in bile duct
(stones)
•Free entry of contrast to the
duodenum
CBD
Duodenum
T-tube
In this case there is no abnormality and the tube can be
pulled out safely. The resulting hole in bile duct closes
spontaneously within 2 days
Normal T-tube cholangiogram
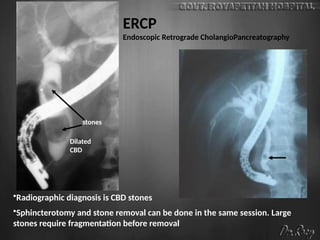
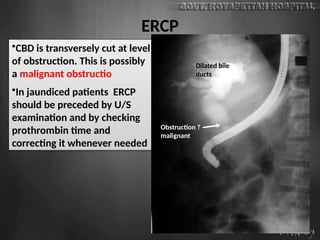
ERCP
•CBD is transverselycut at level
of obstruction. This is possibly
a malignant obstructio
•In jaundiced patients ERCP
should be preceded by U/S
examination and by checking
prothrombin time and
correcting it whenever needed
Dilated bile
ducts
Obstruction ?
malignant
69.
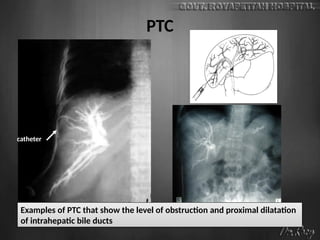
PTC
catheter
Examples of PTCthat show the level of obstruction and proximal dilatation
of intrahepatic bile ducts


































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)

















