Downloaded 19 times


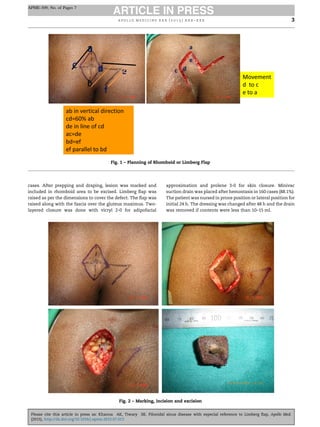





This document discusses pilonidal sinus disease and summarizes the use of the Limberg flap surgical procedure in 180 patients over 10 years. Some key points: - Pilonidal sinus disease commonly affects the hair follicles in the natal cleft, presenting as cysts, sinuses or abscesses. It is more common in males and associated with obesity, sweating and sedentary lifestyles. - The study evaluated 180 patients who underwent rhomboid excision and Limberg flap reconstruction surgery. This procedure aims to thoroughly excise infected tissue and close the wound with minimal complications and recurrence. - Results found a low recurrence rate of 3.3% and minor complications in a small