Download to read offline


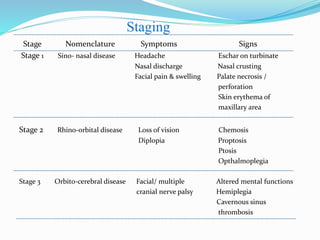
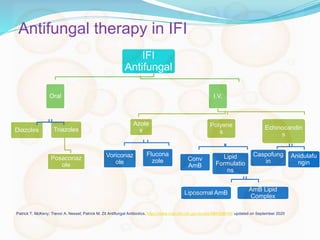




- Mucormycosis is a life-threatening fungal infection caused by fungi of the order Mucorales. It mostly affects immunocompromised individuals, especially those with uncontrolled diabetes. - The document discusses the epidemiology, risk factors, clinical manifestations, diagnosis, and management of mucormycosis. It emphasizes the importance of early diagnosis, aggressive surgical debridement of infected tissues, antifungal therapy typically with amphotericin B, and control of underlying conditions. - Prompt treatment including surgical debridement and antifungal therapy can significantly improve survival rates for mucormycosis compared to antifungal therapy or surgery alone. However, mortality remains high due to












































































