Downloaded 10 times
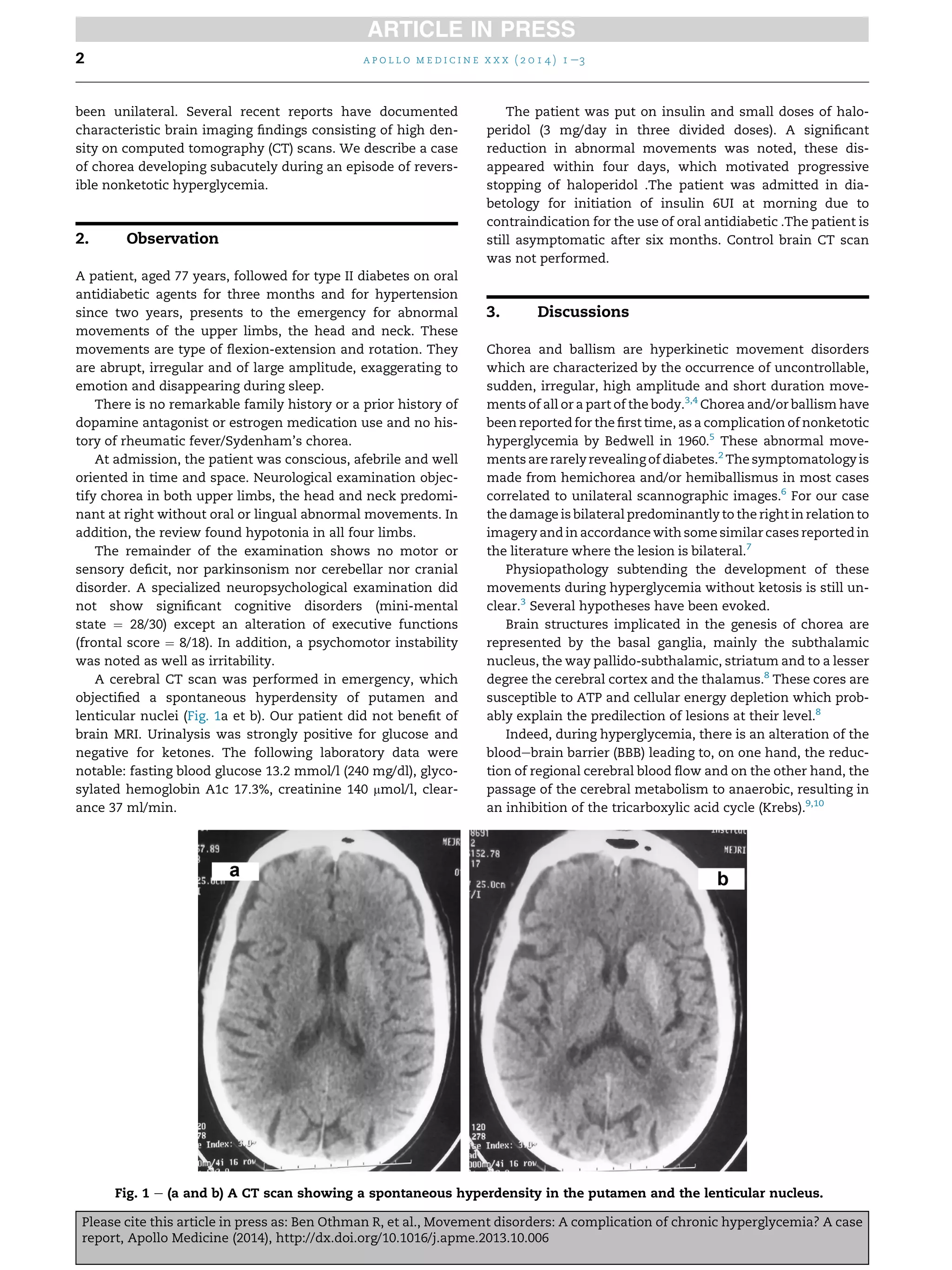



A 77-year-old man presented with bilateral choreic movements that had developed over the past month. He had a history of poorly controlled type 2 diabetes. At admission, he was found to have severe hyperglycemia without ketosis. A CT scan showed hyperdensity in the putamen and lenticular nucleus. Treatment with insulin, haloperidol, and glycemic control led to regression of the choreic movements within 4 days. Chorea secondary to nonketotic hyperglycemia is a rare complication of uncontrolled diabetes that is usually reversible with normalization of blood glucose levels and neuroleptic treatment. The pathophysiology is thought to involve metabolic disturbances from hyperglycemia impairing neurotransmission in basal ganglia structures and























































































