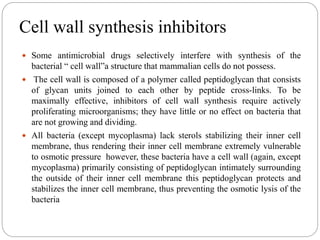
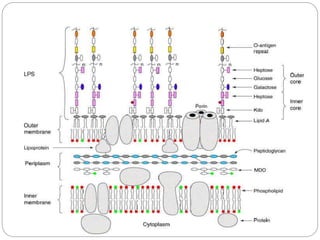
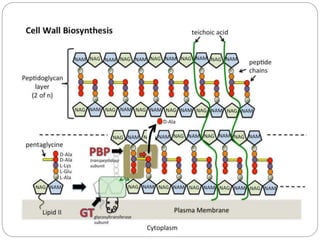
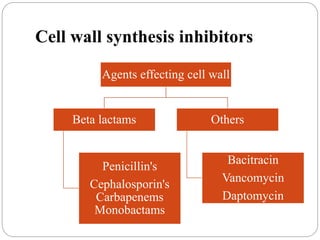
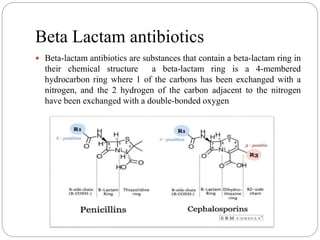
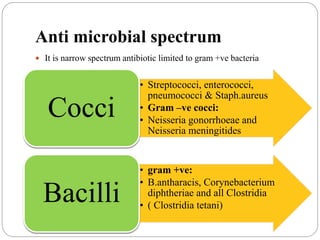
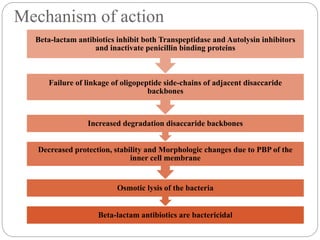
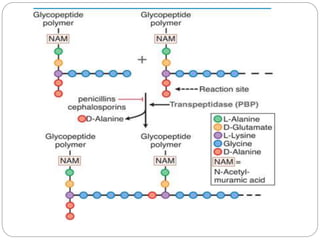
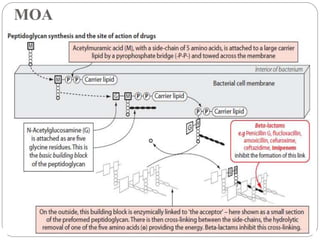
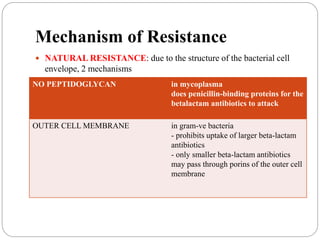
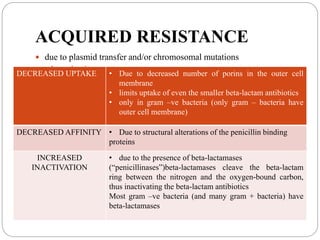
Penicillin and other beta-lactam antibiotics work by inhibiting the penicillin-binding proteins (PBPs) involved in bacterial cell wall synthesis. This disrupts cell wall formation and causes cell lysis and death. While effective against many gram-positive and some gram-negative bacteria, resistance can develop through beta-lactamase production or modifications of PBPs. Different penicillins have varying spectra of activity, pharmacokinetic properties, and resistance profiles that determine their clinical applications.