Downloaded 907 times

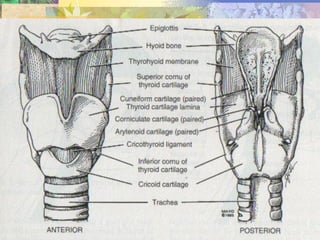

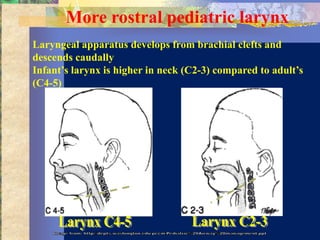
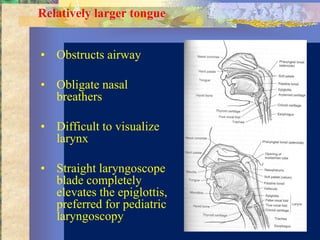
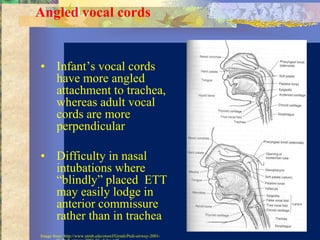
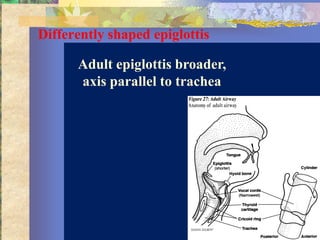
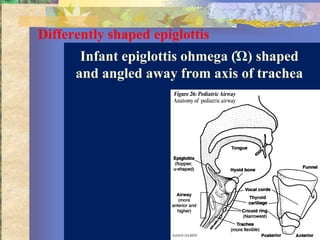
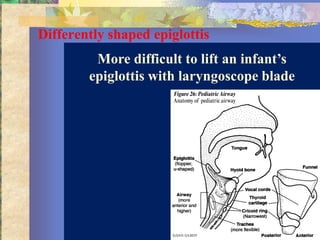
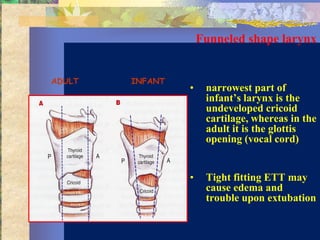
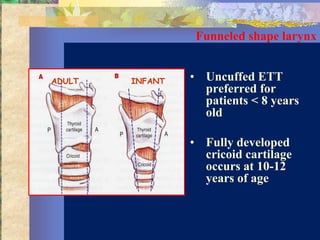
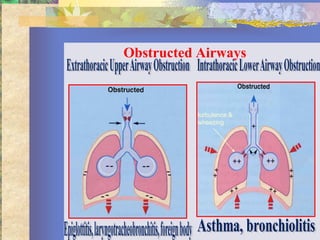
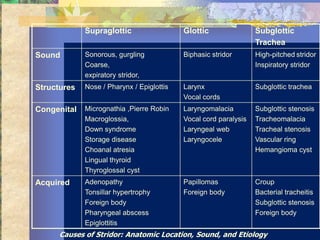



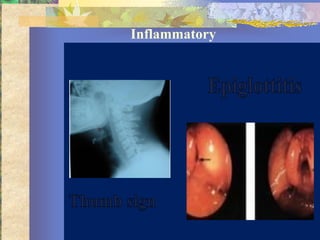


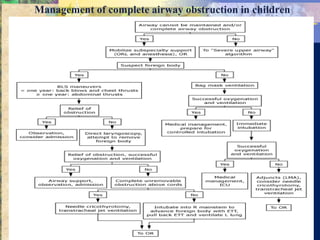
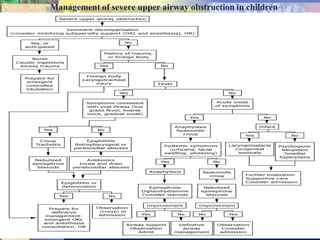

This document discusses the pediatric airway, including normal anatomy, physiology, airway evaluation, and management of normal versus abnormal airways. It notes that the pediatric airway differs from adults in having a more rostral larynx, relatively larger tongue, angled vocal cords, differently shaped epiglottis, and a funneled larynx with the narrowest part being the cricoid cartilage. Proper evaluation of the pediatric airway involves obtaining a thorough medical history and performing a physical exam to identify any signs of impending respiratory failure. Life-threatening causes of acute upper airway obstruction include epiglottitis, retropharyngeal abscess, and foreign body aspiration.






































































































