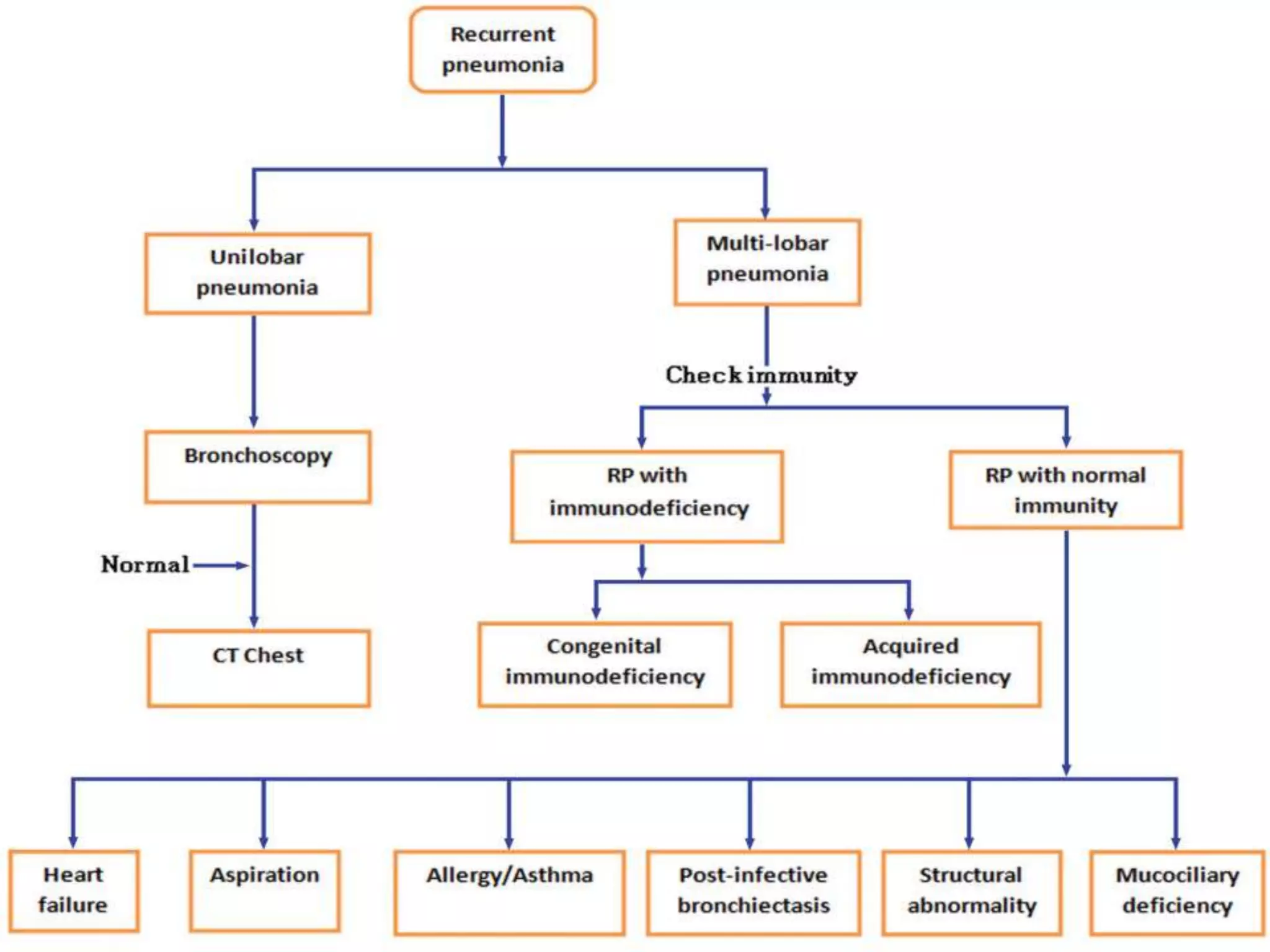
This document provides information on evaluating and diagnosing children with recurrent pneumonia. It discusses obtaining a thorough medical history including details of pneumonia episodes, risk factors, and associated symptoms. A complete physical exam focuses on the respiratory system and signs of underlying conditions. Initial tests include a CBC, chest X-ray, and Mantoux test. Further tests like CT, PFTs, bronchoscopy may help identify structural abnormalities, aspiration, or immunodeficiencies causing recurrent pneumonia. Treatment involves managing the specific illness and providing nutritional/respiratory support.



































































![Community acquired pneumonia [cap] in children](https://cdn.slidesharecdn.com/ss_thumbnails/communityacquiredpneumoniacap-130907093236--thumbnail.jpg?width=640&height=640&fit=bounds)

































