Downloaded 2,259 times



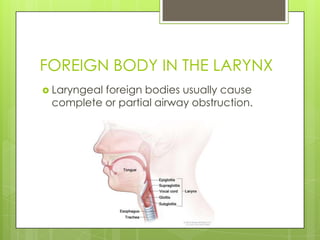

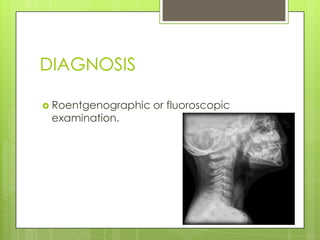
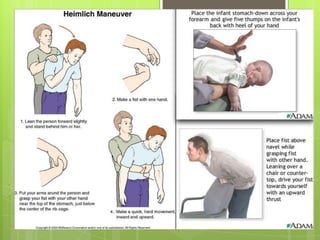


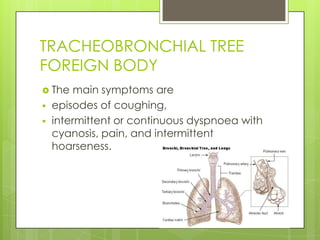


This document discusses airway foreign bodies. Young children ages 1-3 are most at risk of aspirating objects due to lack of teeth and coordination. Common aspirated items include peanuts and other foods. Foreign bodies can lodge in the larynx, trachea or bronchi. Symptoms depend on the location but may include coughing, difficulty breathing or pain. Diagnosis involves history, imaging and examination. Removal requires visualization and extraction, often using laryngoscopy or bronchoscopy under anesthesia.























































































