Downloaded 867 times


![Sokal Index for Chronic Myelogenous
Leukemia (CML) survival
• Sokal Score = exp[0.0116 × (age in years – 43.4)] + [0.0345 × (spleen
size in cm – 7.51)] + [0.188 x ((platelets in 109
/L / 700)2
– 0.563)] +
[0.0887 × (blasts in % – 2.10)]
dr.shumaylaaslam@gmail.com](https://image.slidesharecdn.com/chronicmyeloidleukemia-oncohoure-190601070621/85/Chronic-myeloid-leukemia-CML-28-320.jpg)


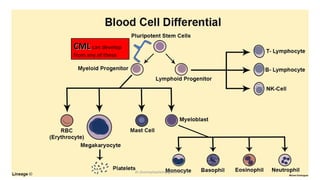
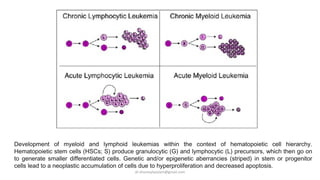
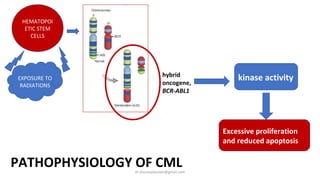
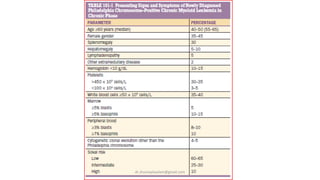
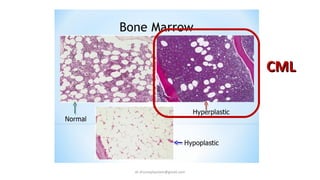
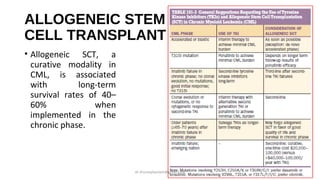
Chronic Myeloid Leukemia (CML) is characterized by the presence of the BCR-ABL1 fusion gene resulting from a translocation between chromosomes 9 and 22, and accounts for about 15% of leukemia cases. The disease progresses through phases, with patients often diagnosed in the chronic phase; treatments like tyrosine kinase inhibitors have significantly improved survival rates. Key factors for prognosis include age, spleen size, and blast percentages, with allogeneic stem cell transplant offering a potential cure during the chronic phase.