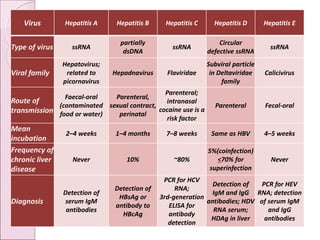
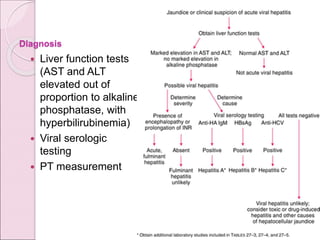
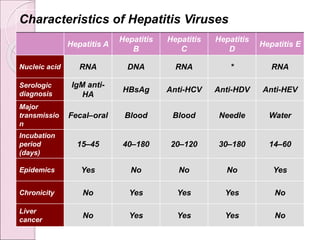
This document discusses various types of viral hepatitis including hepatitis A, B, C, D and E. It describes the causative viruses, modes of transmission, clinical features, diagnosis and potential outcomes of each type of viral hepatitis. Hepatitis A virus causes an acute, self-limiting form of hepatitis while hepatitis B, C and D can potentially lead to chronic liver disease and cirrhosis. Differentiating the types of viral hepatitis requires considering aspects such as incubation period, routes of transmission, risk factors and specific laboratory markers.