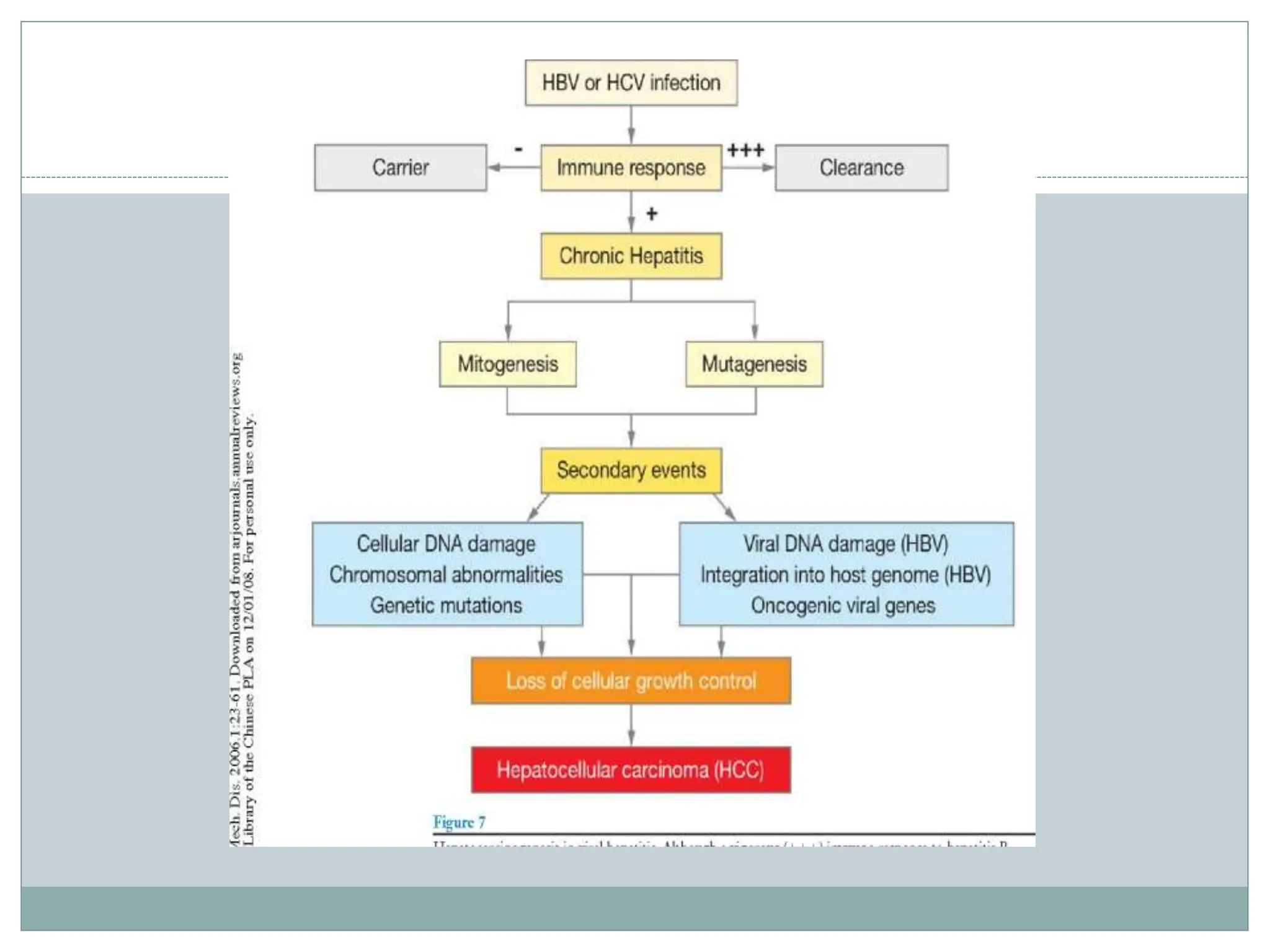
Viral hepatitis is an inflammation of the liver caused by infectious hepatitis viruses. There are 5 main hepatitis viruses - Hepatitis A, B, C, D, and E. Hepatitis A is transmitted through the fecal-oral route while Hepatitis B can be transmitted sexually or parenterally. Hepatitis C is commonly spread through intravenous drug use or blood transfusions. Hepatitis D only infects those also infected with Hepatitis B. Hepatitis E is also spread through the fecal-oral route. Acute viral hepatitis presents with fatigue, nausea, abdominal pain and jaundice while chronic hepatitis from some viruses can lead to cirrhosis or liver cancer over many years.




![HEPATITIS
DEFINITION: Hepatitis is inflammation of the liver that
may result from infectious or other causes.
Examples of hepatitis with infectious causes are viral
hepatitis, infectious mononucleosis, secondary syphilis, and
tuberculosis,etc
Noninfectious hepatitis can result from excessive or
prolonged use of toxic substances (e.g., drugs
[acetaminophen, alcohol, halothane, ketoconazole,
methyldopa, methotrexate]; more commonly,
alcohol),auto-immune](https://image.slidesharecdn.com/hepatitis-240227045304-247b40c3/75/Viral-Hepatitis-disease-pathogenesis-hbsag-5-2048.jpg)