
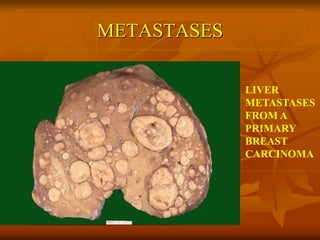



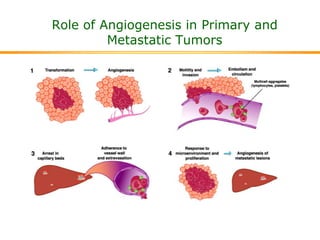

This document discusses tumor metastasis and the pathways involved. It covers: 1. Metastasis occurs when tumor cells spread discontinuously from the primary site to distant organs. More aggressive tumors are more likely to metastasize. 2. Tumor cells can spread via lymphatic vessels, hematogenous spread through the bloodstream, or by seeding body cavities. The most common route is lymphatic spread for carcinomas and hematogenous spread for sarcomas. 3. The metastatic process involves tumor progression, invasion of surrounding tissue, entry and survival in the bloodstream, arrest at distant sites, extravasation, and colonization of secondary tumors. Specific adhesion molecules and chemotactic


![Neoplasia [part 1]](https://cdn.slidesharecdn.com/ss_thumbnails/neoplasiapart1-190918152450-thumbnail.jpg?width=640&height=640&fit=bounds)


































































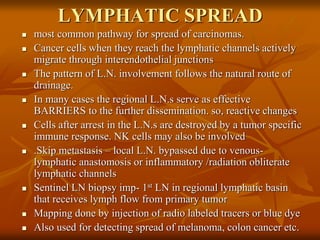
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

















