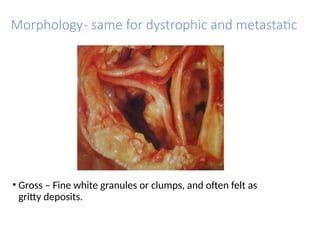
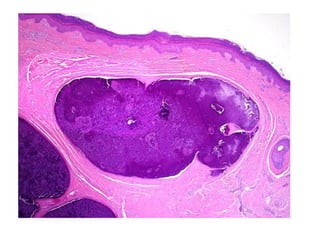
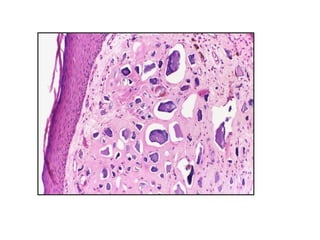
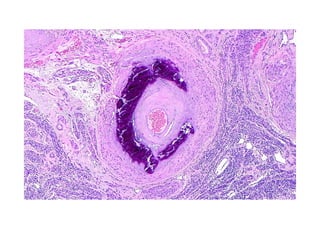
Pathological calcification involves abnormal calcium salt deposition in tissues, categorized into dystrophic and metastatic calcification. Dystrophic calcification occurs in dead or degenerating cells despite normal serum calcium levels, while metastatic calcification arises from hypercalcemia due to increased serum calcium or metabolic disorders. Both types exhibit similar morphological features, including fine white granules and a basophilic granular appearance under microscopic examination.