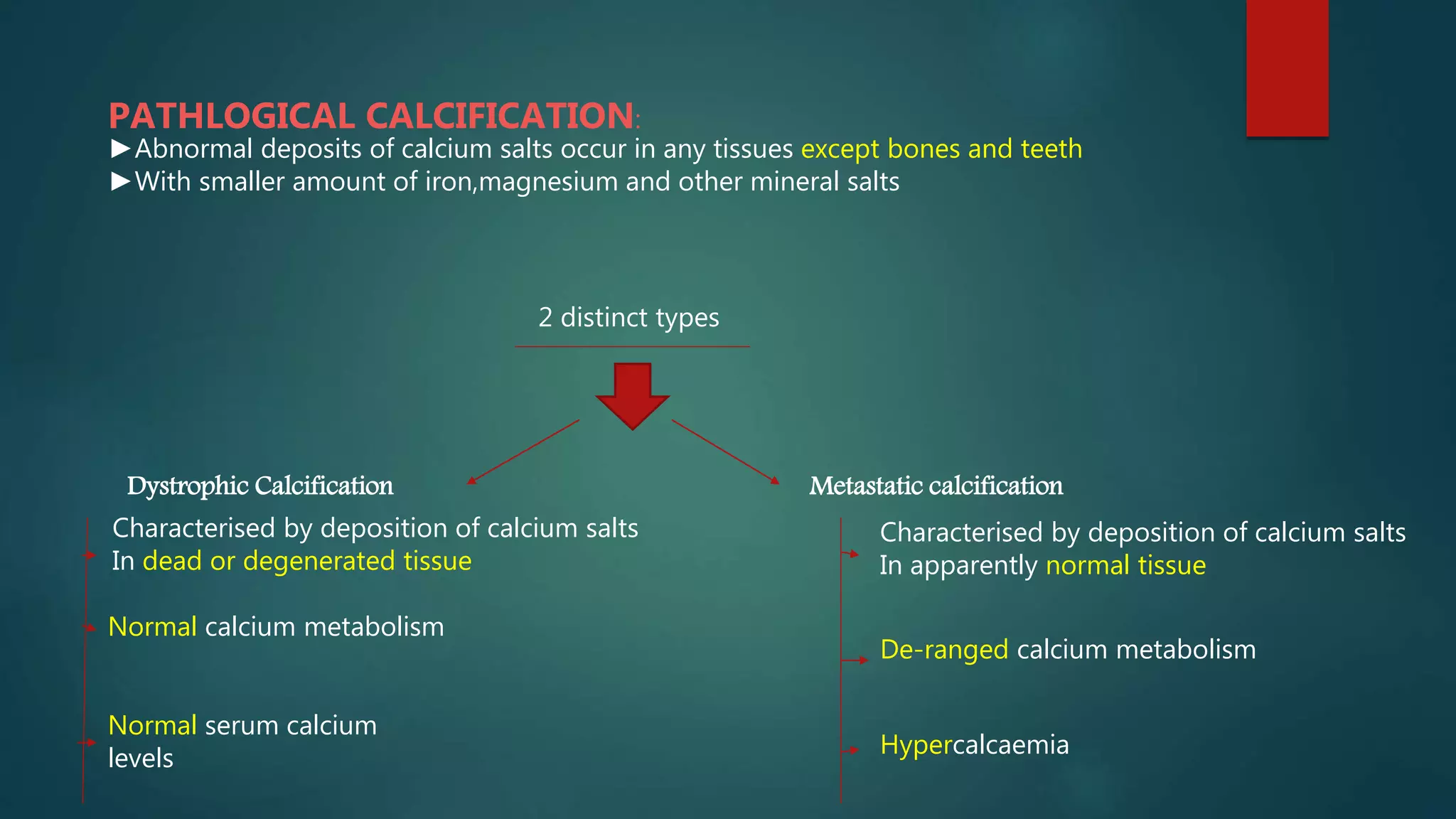
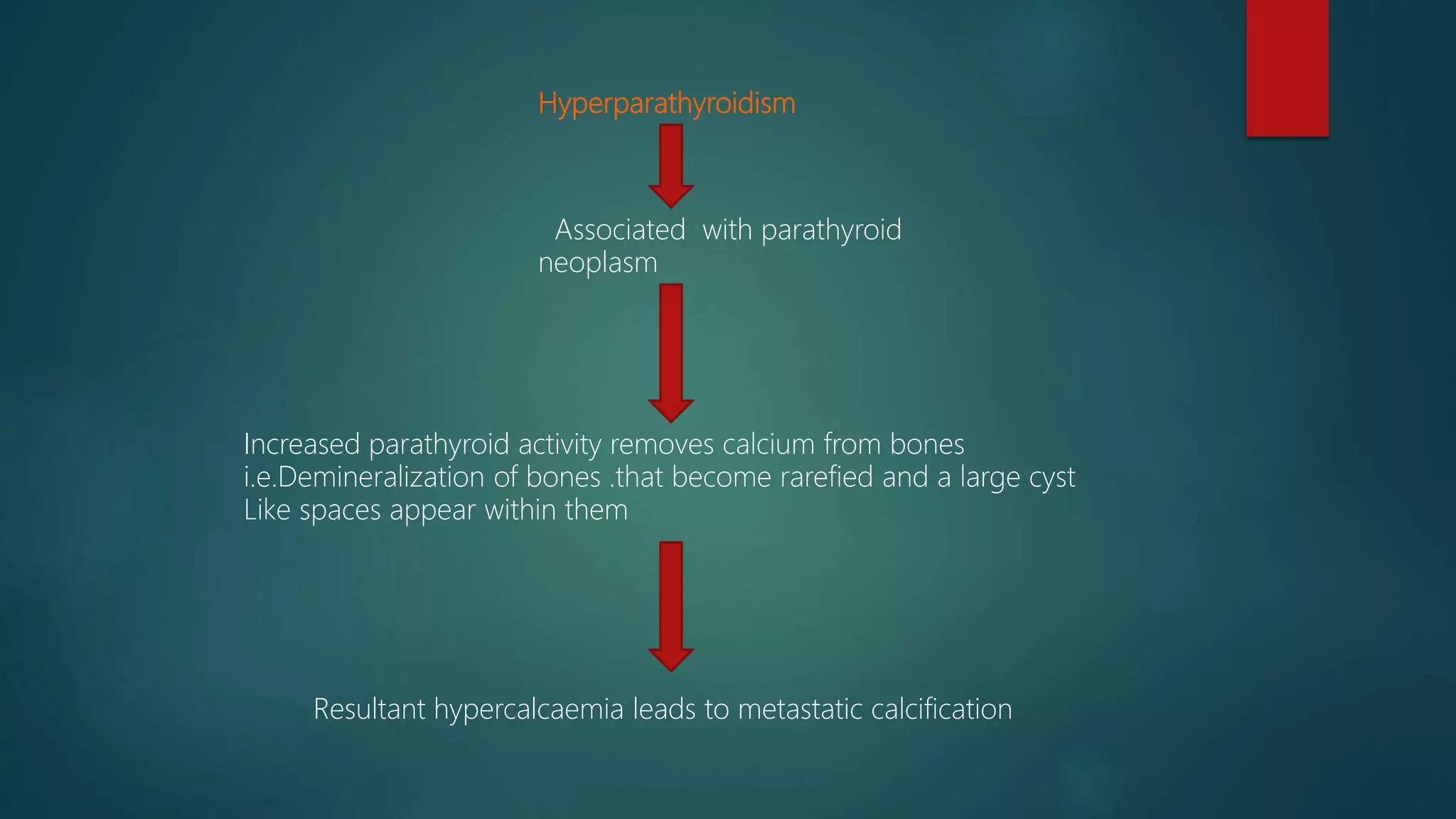
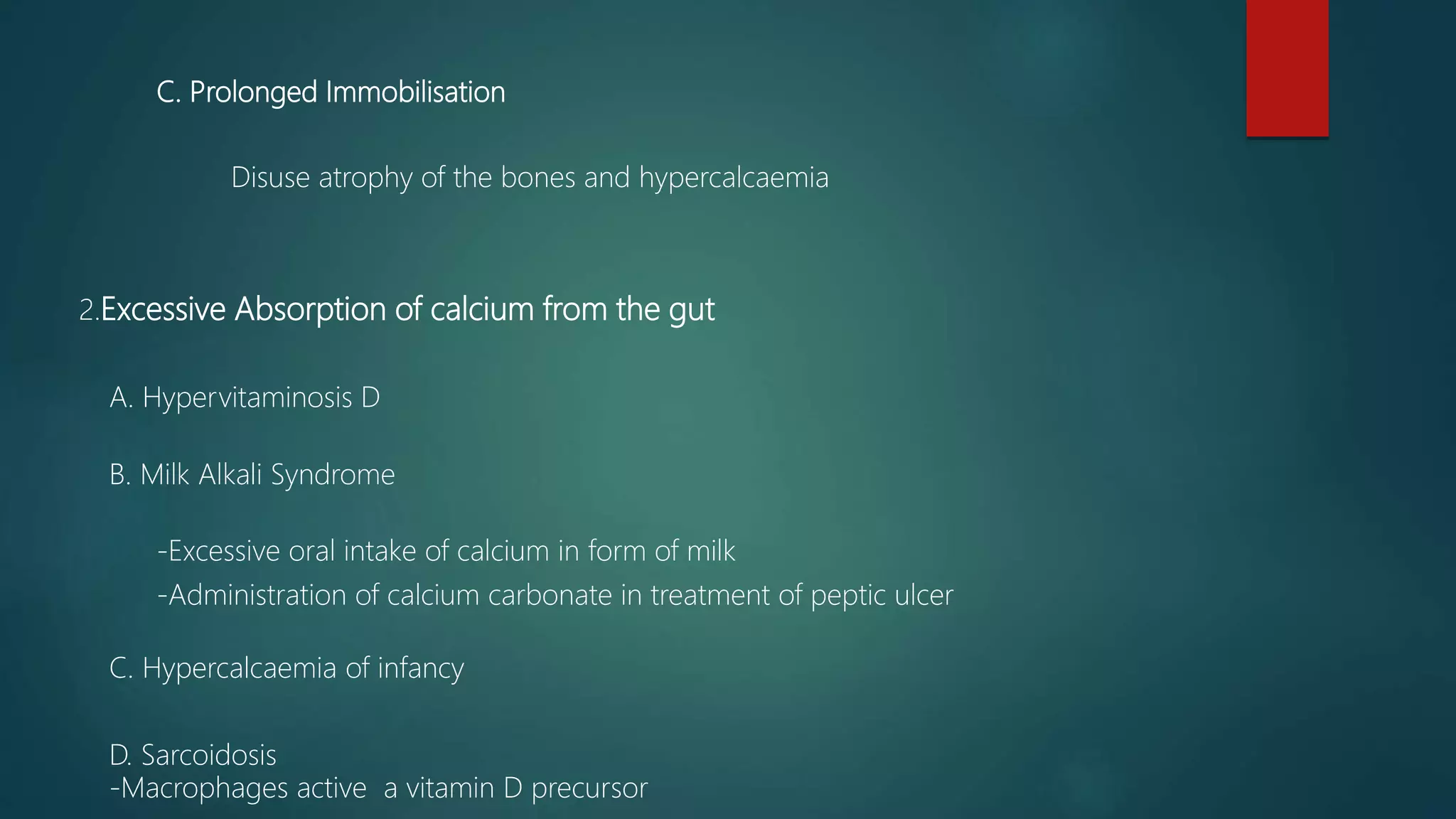
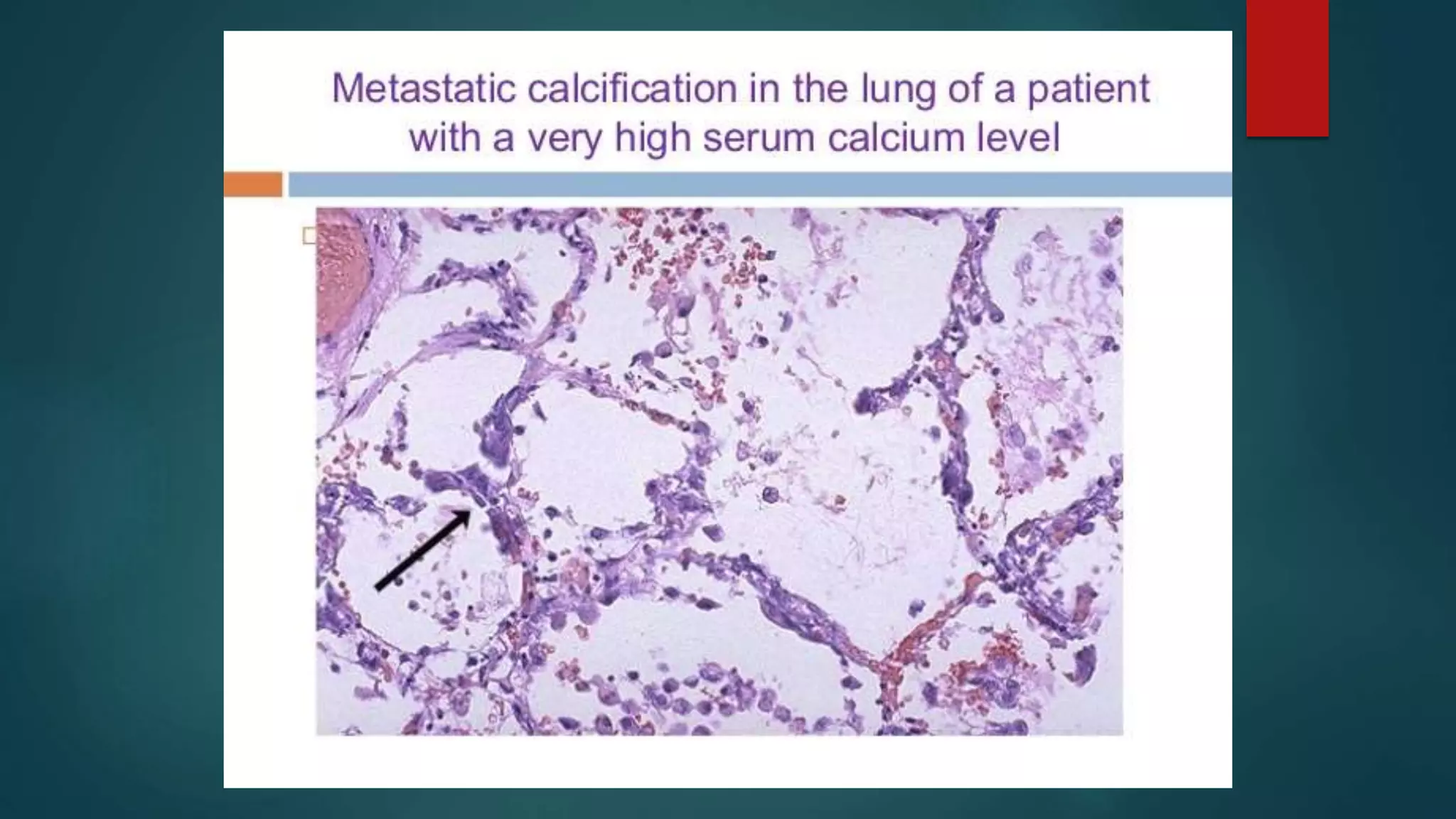
This document discusses pathological calcification, which occurs when calcium salts abnormally deposit in tissues other than bones and teeth. There are two types: dystrophic calcification, which occurs in dead or damaged tissues; and metastatic calcification, which occurs in normal tissues due to disorders of calcium metabolism. Metastatic calcification is usually reversible if the underlying metabolic disorder, such as hyperparathyroidism or hypercalcemia from kidney failure, is corrected. Common sites of metastatic calcification are the kidneys, lungs, blood vessels, stomach, and cornea. Under the microscope, calcium salt deposits appear as basophilic granular clumps that can be confirmed with special staining techniques.