Downloaded 317 times


![It is the persistent vascular connection between the
pulmonary artery and the aorta. functionally, the closure of
ductus arteriosus [which is normally present in fetal life]
occurs soon after birth. when ductus arteriosus remains
patent and open after birth, the blood flows in the ductus
from the aorta to the pulmonary artery due to higher
pressure in the aorta](https://image.slidesharecdn.com/patentductusarteriosus-150729125502-lva1-app6892/85/Patent-ductus-arteriosus-2-320.jpg)
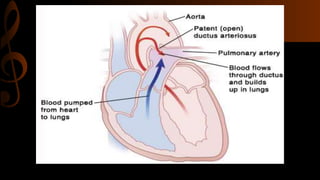


Patent ductus arteriosus (PDA) is the persistent opening of the ductus arteriosus after birth, allowing blood to flow from the aorta to the pulmonary artery. It is common in preterm infants under 1.5kg. Untreated PDA can lead to pulmonary overload and congestive heart failure. Symptoms include tachypnea, bounding pulse, and frequent respiratory infections. Diagnosis involves physical exam, chest x-ray, echocardiogram, and cardiac catheterization. Treatment options include medications to close the ductus like indomethacin or surgery to ligate the ductus if medications fail or for symptomatic patients. Complications can include congestive heart failure, infective end



























































![Patent ductus arteriosus [PDA], shane stanley.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/patentductusarteriosuspdashanestanley-251016112835-ae3342d7-thumbnail.jpg?width=640&height=640&fit=bounds)



















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












