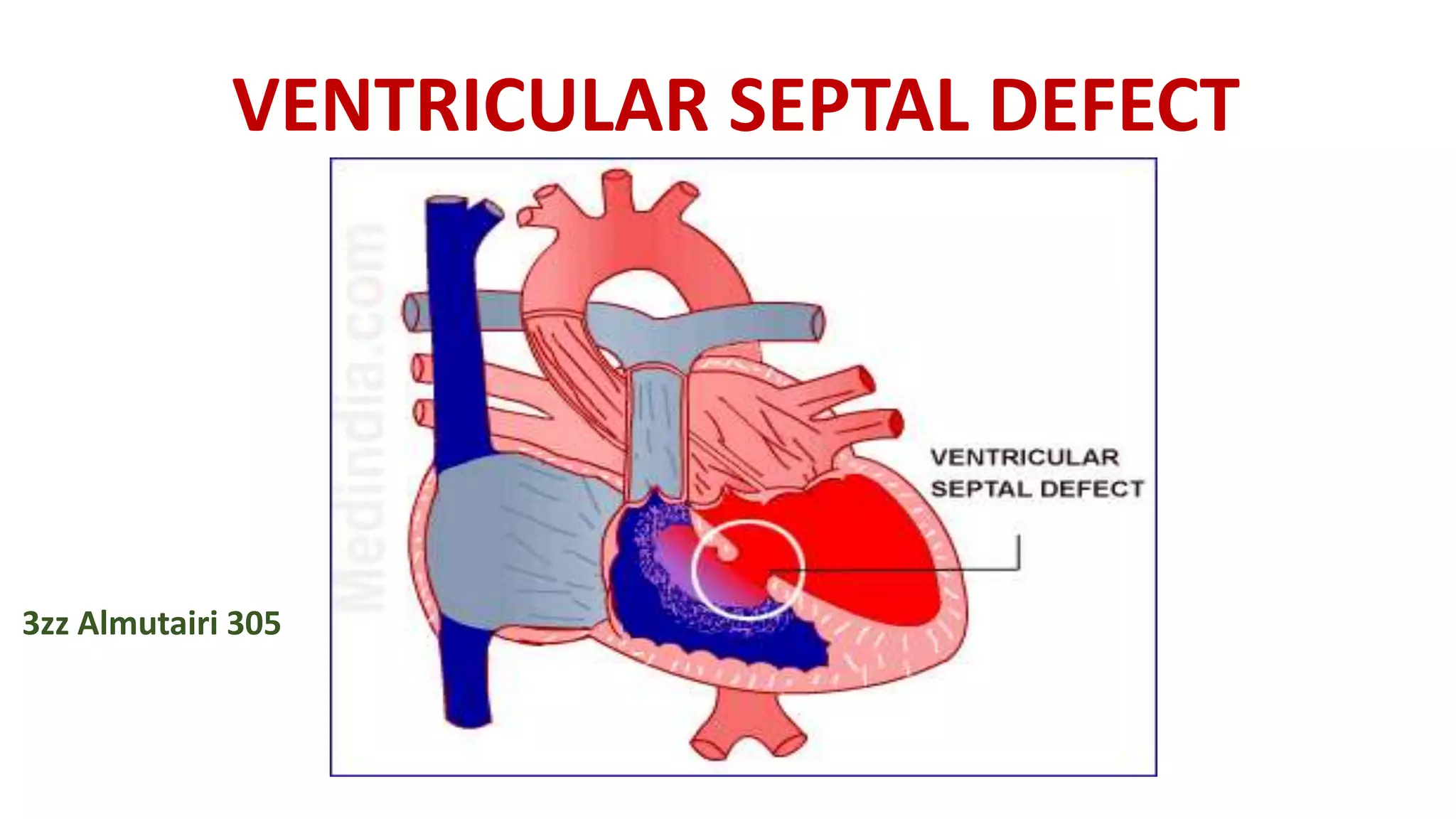
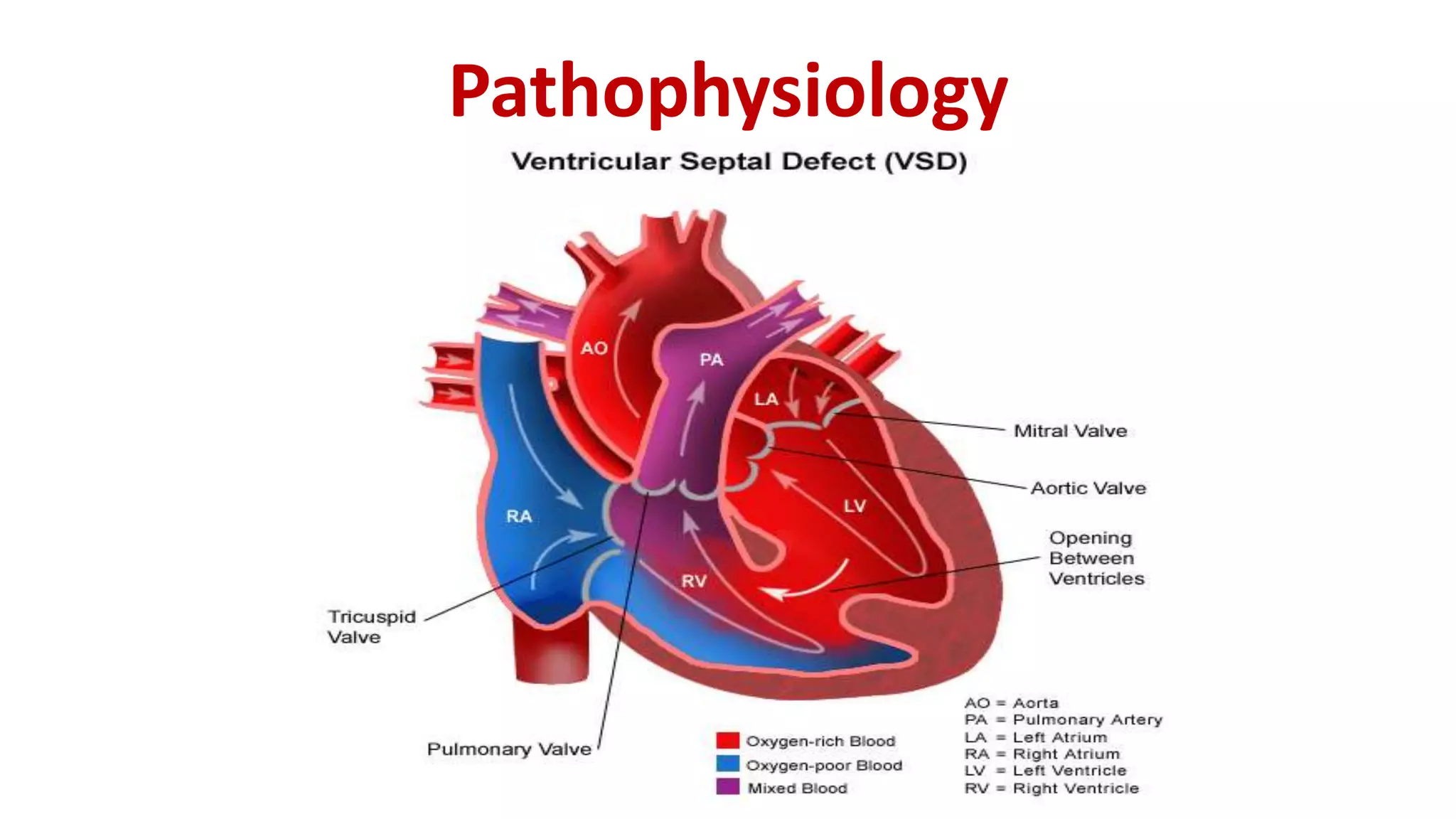
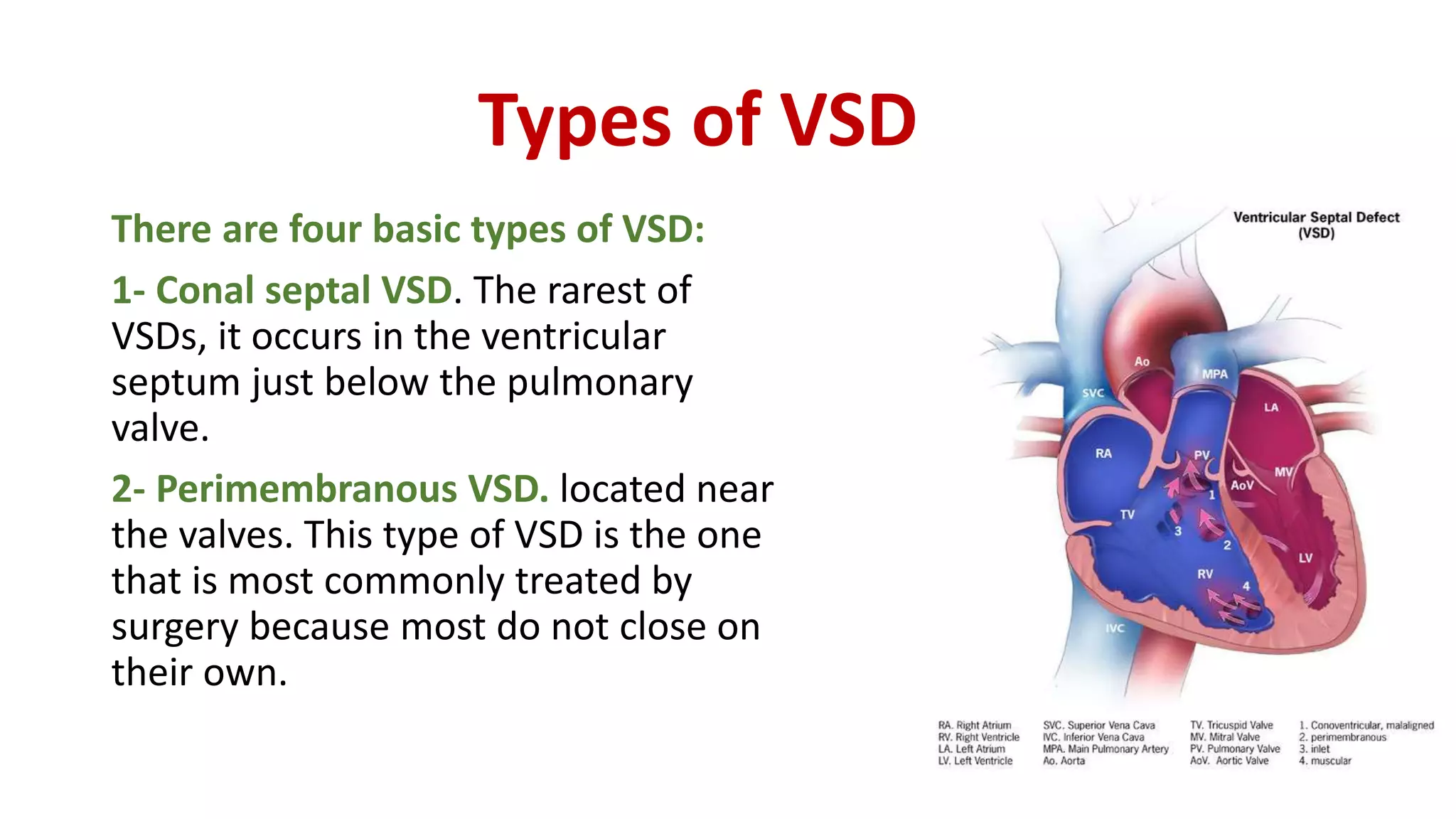
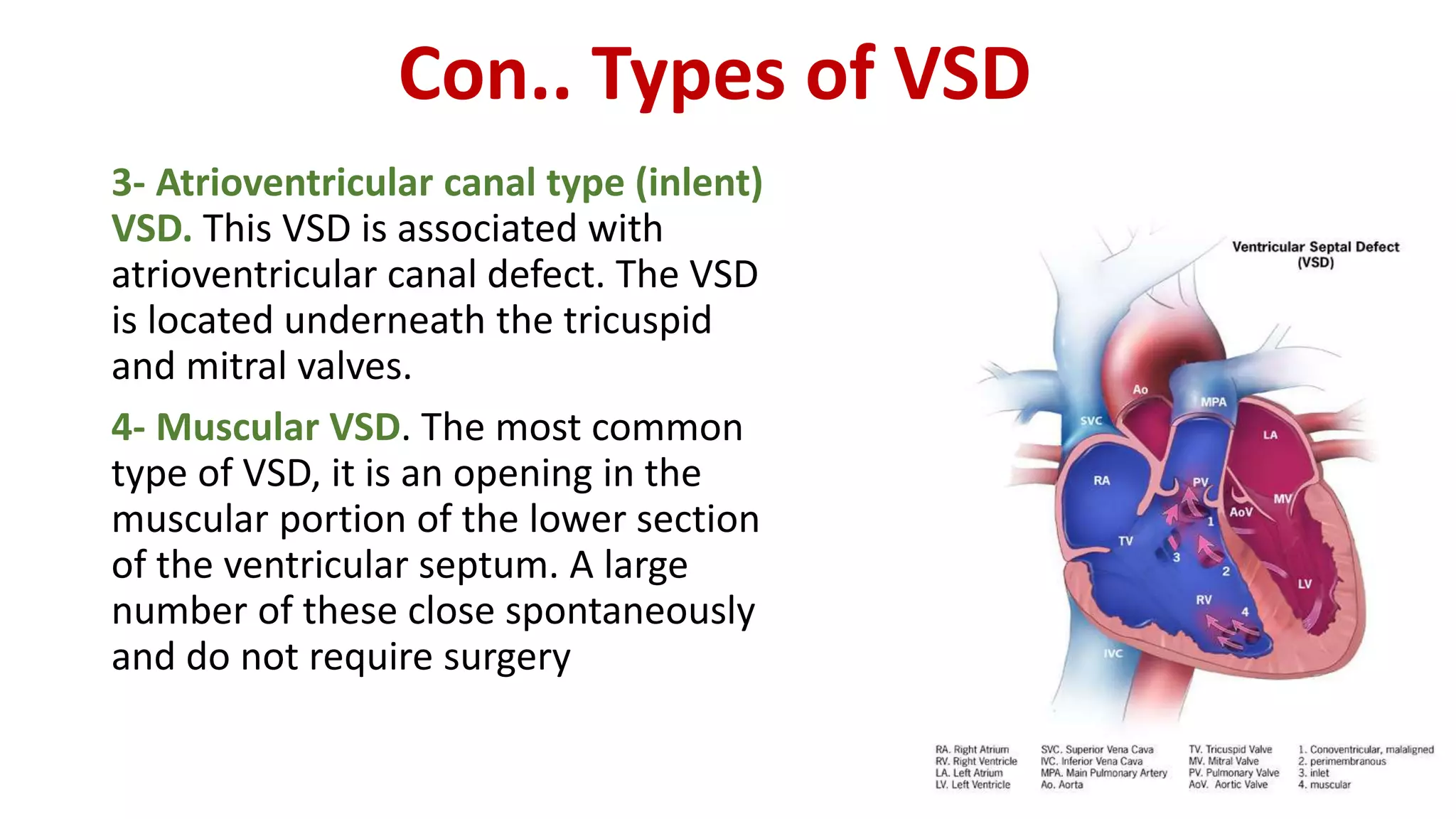
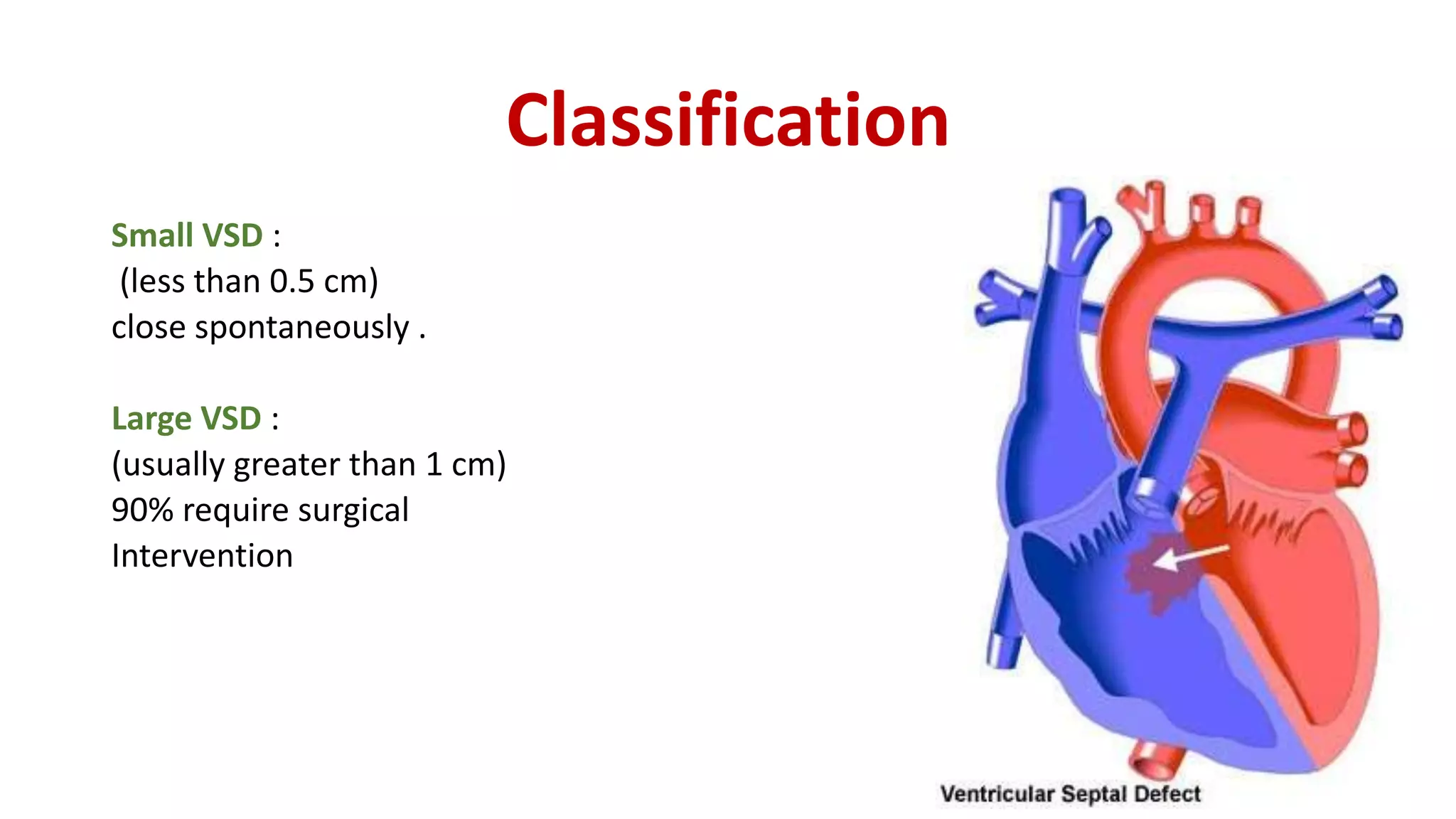
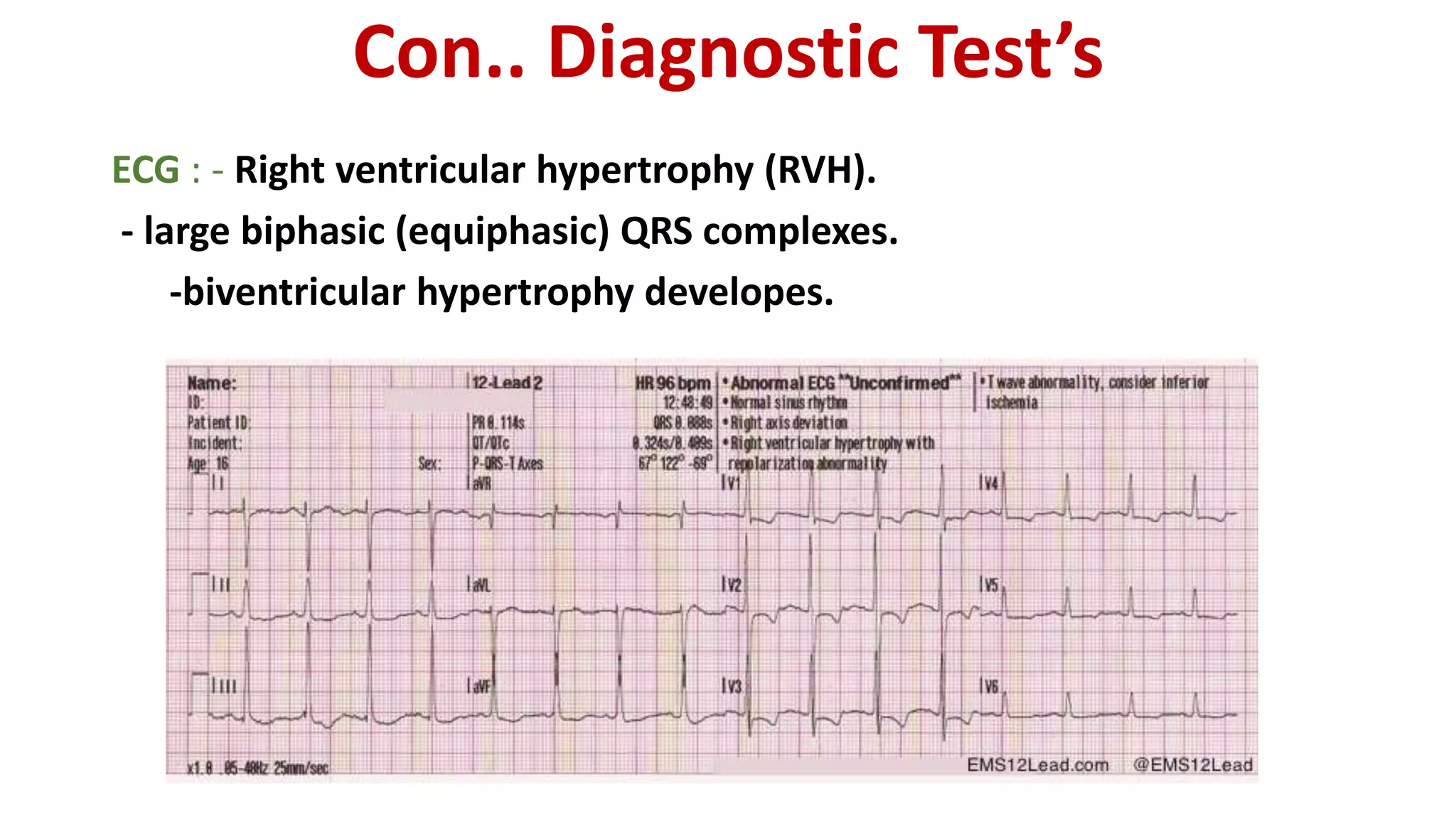
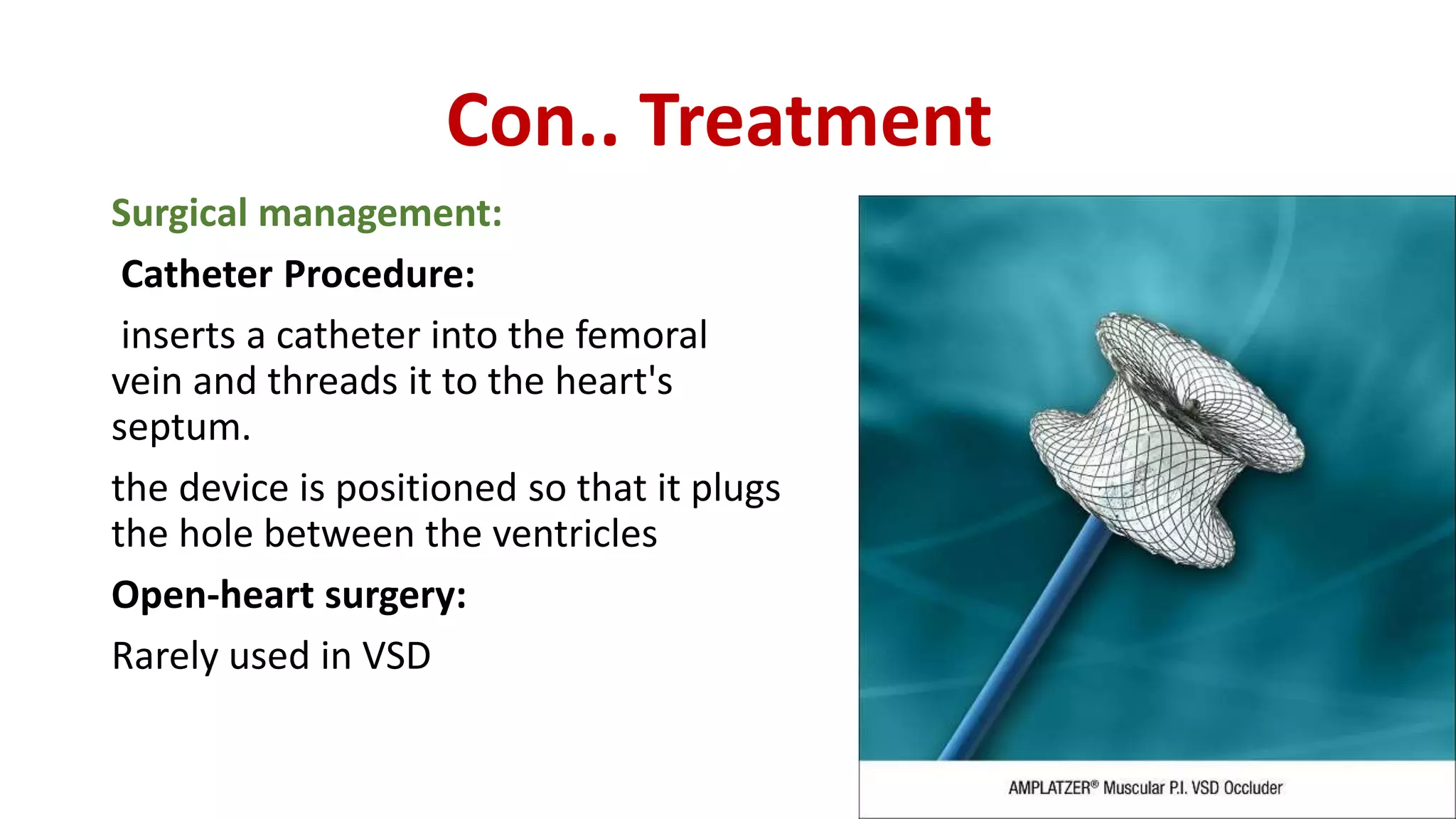
Ventricular septal defect (VSD) is a congenital heart defect where there is an abnormal opening in the wall separating the left and right ventricles of the heart. There are four main types of VSD. VSDs can be small or large depending on size, and large VSDs typically require surgical closure. Symptoms include heart murmur, fatigue, sweating, and cyanosis. Echocardiogram and ECG are used for diagnosis. Treatment involves medication for heart failure symptoms or closure of the defect via catheterization or open-heart surgery. Post-operative nursing care focuses on monitoring for dysrhythmias and improving cardiac output and gas exchange.